Download
1 / 79
790 likes | 1.03k Views
Shoulder Problem Evaluation. MS3 Family Medicine. Second most common musculoskeletal complaint Difficult joint to examine Multidirectional range of motion- UNIQUE! Shoulder injury can affect nearly every sport and many daily activities. Objectives. Review pertinent anatomy

E N D
Shoulder Problem Evaluation MS3 Family Medicine
Second most common musculoskeletal complaint • Difficult joint to examine • Multidirectional range of motion- UNIQUE! • Shoulder injury can affect nearly every sport and many daily activities
Objectives • Review pertinent anatomy • Discuss common pathology • Discuss historical clues to diagnosis • Select cases • Physical exam in small group discussions
Where do things go wrong??Dislocations and Separations Dislocations and separations are protected by both “static” and “dynamic” stabilizers…
Where do things go wrong??Dislocations and Separations Oh, yeah…Arthritis can happen at these joints, too…
Glenohumeral Joint • Shallow (“golf ball sitting on a tee”) • Inherently unstable (maximizes ROM) • Static stabilizers • glenohumeral ligaments, glenoid labrum and capsule • Dynamic stabilizers • Predominantly rotator cuff muscles • Also scapular stabilizers • Trapezius, leavator scapulae, serratus anterior, rhomboids
What goes wrong…Besides separations and dislocations?? Instability!!!
SupraspinatusABD InfraspinatusER Teres minor ER Supscapularis IR The Rotator Cuff Muscles: SITS Depress humeral head against glenoid to allow full abduction
What can go wrong??? Impingement!!!!!!!
Deltoid Rotator cuff Teres major Latissimus dorsi Biceps Pectoralis muscles Other Anatomy
Don’t forget the scapular stabilizer muscles
So…what causes shoulder pain? • Impingement • Labrum and biceps pathology • A-C joint pathology • Rotator Cuff Injury • Instability Among other things…
Clinical ExamHistory • Pain • Acute • Chronic • Weakness • Deformity
Clinical ExamHistory • Single event • Repetitive overload • Instability • Does it feel like it’s going to come out? • Catching/Locking
Clinical ExamHistory • Sport / Occupation • Previous injury • Previous treatment • Other joints involved • Disability
Physical Exam: Big 6 • Inspection • Palpation • Range of Motion • Strength • Neurovascular • Special Tests
Special Tests Impingement Rotator Cuff Integrity Labrum and Biceps AC (SC) Joints Instability
Physical Exam • The physical exam will be demonstrated during small group discussions…
0 Which rotator cuff muscle(s) are responsible for external rotation • Supraspinatus • Infraspinatus • Subscapularis • Teres Minor • Both 2 and 4
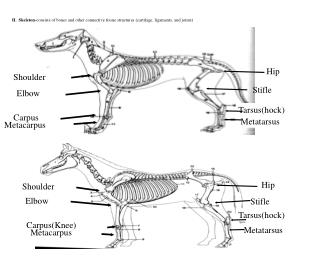
:00 The apex (bottom) of the scapula is at what level of the spine? • C7 • T3 • T7 • T12 • L4
Case #1 • 22-year-old male rugby player falls onto his right shoulder while being tackled • Severe pain on top of his right shoulder
Case #1 • Notable deformity over superior shoulder • Painful range of motion • Unable to lift right arm above waist • Special Tests?? • Diagnosis???
Acromioclavicular (A-C) Sprain • Special Tests • Shear Test • Cross Arm Test • A-C Palpation • Resisted Extension • Active compression test
Acromioclavicular (A-C) Sprain • Damage to A-C joint ligaments • Pain and/or deformity over A-C joint • Graded I-VI • I-III usually treated non-operatively • IV-VI referred to orthopedic surgery
AC Joint Sprain Treatment • Analgesics, ice prn • Sling for as long as needed • Physical Therapy • ROM restoration • Gradual strength exercise • Return to sport activity as tolerated
Case #2 • 24-year-old male handball player • Fell onto his shoulder after being pushed • Intense pain • Hand is tingling and arm feels like it’s hanging • X-rays
X RAYS DIAGNOSIS???
Shoulder Dislocation/Anterior Instability • Humeral head dislocates from glenoid fossa • Almost always anterior (95%) • Usually traumatic with injury to capsule-labrum complex
Shoulder Dislocation/Anterior Instability • Treatment • Reduction of dislocation • Protection & rehab, rehab, rehab • Most will have future dislocations and/or instability • At least 70%!!! (young) • May require surgical tightening/repair of the capsule/labrum complex
Special TestsGlenoid Labrum and Instability • Biceps Load I and II • Kim Test • Jerk Test • Active-Compression Test (O’Brien) • Crank Test • Apprehension Test • Relocation Test • Load and Shift • Sulcas Sign
30 10 0 0 Which of the following structures can be “impinged”? • Biceps tendon • Subacromial Bursa • Rotator Cuff Tendons • All of the above
Case #3 • 35-year-old male tennis player • Shoulder pain exacerbated by practicing serves • Develops dull, aching pain in right shoulder
SHOULDER PAINPhysical Exam • Tenderness to palpation anterior shoulder • Pain with abduction starting around 90 degrees • Unable to lift arm past 120 degrees • Pain with forward flexion at 90-120 degrees • Special Tests??? Diagnosis???
Shoulder PainPhysical Exam Hawkin’s positive Neer’s positive IMPINGEMENT???
Impingement as a Clinical Sign • Repetitive overhead activities • Subacromial bursa and/or rotator cuff impinged between acromion & humerus • Physical therapy, activity modification +/- medications
Diagnoses associated with clinical sign of Rotator Cuff Impingement: • Subacromial bone spurs and / or bursal hypertrophy • AC joint arthrosis and /or bone spurs • Rotator cuff disease • Superior labral injury • Glenohumeral instability • Scapular dyskinesis • Biceps tendinopathy A diagnostic injection sometimes helps to clarify the diagnosis
Case #4 • 45-year-old weight lifter • Caught bar as it was falling off his shoulder • Sudden pain • Severe weakness left shoulder • Worse with overhead activities; while sleeping at night • Pain in anterior lateral shoulder • Special tests?
Case #4 Drop Arm Test Positive External Rotation Lag Sign positive Weakness with Empty Can Sign Normal bear hug and belly press tests… Diagnosis?????
Rotator Cuff Tear • Supraspinatus tendon most common • Acute trauma or chronic tendinopathy • Treatment dependent upon age/activity • Young, active usually require operative treatment • Older, low-activity usually respond to non-operative treatment