Download
1 / 24
250 likes | 448 Views
Back and Hip Pain. M. Andrew Greganti, MD. Back Pain. Accounts for 2.5% of medical visits – second most common reason for office visits in US Prevalence varies widely – 1.2 to 43% Risk factors: Obesity Smoking Female gender Physically strenuous or sedentary work – lifting over 25 lbs

E N D
Back and Hip Pain M. Andrew Greganti, MD
Back Pain • Accounts for 2.5% of medical visits – second most common reason for office visits in US • Prevalence varies widely – 1.2 to 43% • Risk factors: • Obesity • Smoking • Female gender • Physically strenuous or sedentary work – lifting over 25 lbs • Low educational level • Job dissatisfaction • Somatization disorder, anxiety, depression • Workers’ Compensation Insurance • Genetic background • Cultural differences
Prognosis • Generally good, especially if expectation is to improve – most do get better with no intervention • Less than 5% have serious underlying pathology • A cause can be found only in a minority of patients • Chronicity seems to correlate with: • Female gender • Increasing age • Pre-existing psychosocial factors
Clinical Evaluation • Key concepts: • Most patients have mechanical low back pain – no infectious, inflammatory, or neoplastic cause. • Degenerative disc disease plays a substantial role but exactly how much of one is unclear. Many patients without pain have discs on MRI. • Muscular and ligamentous sources of pain are probably equally important. • Tender fibro-fatty nodules (back mice) may play some role but correlation with back pain remains in question.
History • Consider 3 major concerns: • Evidence for a systemic process – hx of cancer, age over 50, weight loss, nocturnal pain, unresponsiveness to Rx • Evidence for neurologic compromise – caudaequina syndrome, radiation of pain below the knee, pseudoclaudication as in spinal stenosis, focal weakness • Social or psychological distress contributing to chronic, disabling pain
Physical Examination • Check for spinal curvature – kyphosis, scoliosis, etc. • Check for spinal tenderness • Straight leg raising and crossed straight leg raising • Evaluate for deficits in L4, L5, and S1 distributions. • Lymph node, breast, and prostate exams if neoplasia is suspect • Check peripheral pulses
Diagnostic Imaging • Imaging is essential in these situations: • Progression of neurological findings • History of trauma • History of neoplasia • Age <18 or >50 • Special situations: • Injection drug use • Immunosuppression • Indwelling Foley catheter or recent GU procedure • Concomitant steroid use
Plain Films, MRI, CT • If symptoms persist for 4 to 6 wks with no improvement, order two views of plain films without obliques • Implications of spondylosis, spondylolisthesis, spondylolysis • Order MRI or CT to evaluate progressive neurologic deficits, to evaluate for cancer, or to evaluate patients with refractory symptoms – greater than 12 wks of persistent pain
Treatment of Back Pain • Bed rest is not indicated – may actually delay recovery • NSAIDS and narcotics have similar efficacy – use of NSAIDS should be limited to 2 to 4 wks • Adverse effects more common in older patients • Acetaminophen is probably as good as NSAIDS. • Muscle relaxers are more effective than placebo for short-term relief • NSAIDS + muscle relaxants may be better - based on observational data.
Treatment of Back Pain • Opioids are effective in acute back pain but obviously have multiple side effects and are addicting • Tramadol is a non-opioid and works on the opioid receptor – is worth a trial. • Oral glucocorticoidsprobably are not beneficial for acute pain. • Lidocaine patches, anticonvulsants, antidepressants are of limited effectiveness in acute pain.
Treatment of Back Pain • Epidural injection: • Efficacy remains unclear – conflicting results from controlled trials • Probably best in radiculopathy secondary to HNP – has short-term (at 6 wks) but no long-term benefit at 3 , 6, or 12 months • Not of proven benefit in spinal stenosis and nonspecific pain • No difference in translaminar, transforaminal, and caudal approaches • 2 of 7 trials found epidural injection vs placebo associated with lower rates of subsequent surgery. • Adverse events: dural puncture, bleeding, infection
Treatment of Back Pain • Local or trigger point injection rarely works • Facet joint steroid injection doesn’t help at 1 and 3 months • Medial branch of dorsal ramus nerve blocks are of unknown efficacy • Sacroiliac joint steroid injection was more effective than anesthetic injection in one small trial • Probably does work for spondyloarthropathies • Rx effectiveness of piriformis syndrome using injected steroids remains unclear
Treatment of Back Pain • Chemonucleolysis for HNP should only be used in patients who do not want surgery – not often done in US • Paravertebralbotulinum toxin injection was superior to placebo at 3 and 8 weeks • Evidence for the efficacy of radiofrequency nerve ablation remains inconsistent – would only consider in the most refractory situations • Prolotherapy should not be used
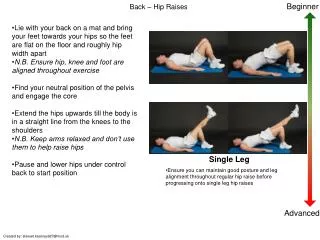
Treatment of Back Pain • Exercise is not good for acute pain in contrast to more chronic pain. • Encourage mobilization as soon as possible. • Physical therapy is, in general, very helpful but no difference in heat/cold, ultrasound, electrical stimulation • TENS effectiveness is very questionable at best. • Spine manipulation by chiropractors may be helpful. • Accupuncture is probably equivalent to NSAIDS. • Traction does not help lumbar pain.
Hip Pain • Basic issues: • The major dilemma is to differentiate among gluteus medius superficial and deep bursitis and osteoarthritis • The hip is “fixed” by the pelvic girdle, making it more difficult to differentiate pain originating in the lumbar spine and knee from hip pain. • The gluteus medius and gluteus minimus muscles abduct the hip and attach at the greater trochanter. • The gluteus maximusextends the hip and attaches just distal to the greater trochanter • The iliopsoas muscle, the major hip flexor, attaches at the lesser trochanter.
Clinical Presentation of Hip Pain • Hip pain with weight bearing and improvement with rest is most compatible with DJD. • Constant pain and pain while supine are more likely with infectious, inflammatory, and neoplastic processes. • Lateral hip pain is often from the joint or from the greater trochanteric bursa, especially if there is point tenderness. • Hip joint pain is more often anterior • Lateral paresthesias raise the possibility of meralgiaparesthetica.
Clinical Presentation of Hip Pain • Anterior hip or groin pain is most often seen in DJD of the hip joint. • Important to differentiate DJD from osteonecrosis • If not worse with repetitive hip flexion, have to consider inguinal hernia and intraabdominal process. • Anterior thigh pain just above the knee presents the most difficulty • Posterior hip pain is not usually from the hip. More commonly is secondary to lumbar disc, sacroiliac disease, facet joint disease.
Clinical Presentation of Hip Pain • Trochanteric bursitis is caused by exaggerrated movement of the gluteus medius tendon and tensor fascia lata over the lateral femur. • More likely to develop with leg length discrepancy, knee arthritis, ankle sprain, LS spine stiffness • Point tenderness over trochanteric bursa • Hip DJD presents with groin pain worse with movement, limited internal rotation (<15 º), limited flexion (<115 º) • Osteonecrosis presents in the groin, thigh, or buttock • Rest pain is common as is nocturnal pain
Hip Examination • Observe patient’s gait - ? antalgic, short leg limp, Trendelenburg gait • Passive internal and external rotation - ? endpoint stiffness – endpoint pain raises osteonecrosis, occult fracture, acute synovitis, metastatic disease • Fabere or Patrick test • Straight leg raising to evaluate lumbar origin • Check sensation lateral thigh - ? meralgia • Evaluate L4, L5, and S1 nerve root distribution • Check for tenderness over the sacroiliac joint • Check leg pulses
Evaluation of Hip Pain • AP of pelvis and hip films • MRI if occult hip or pelvic fracture is suspected – also to evaluate early osteonecrosis • Local anesthetic blocks of sacroiliac joint, trochanteric area below gluteus medius tendon, lateral femoral cutaneous nerve
Treatment of Hip Pain • Very similar to Rx of back pain • Acetaminaphen, tramadol, NSAIDS • Physical therapy • Joint replacement