Download
1 / 65

E N D
Odontogenic sinusitis: classification, etiology, pathogenesis, clinical features, differential diagnosis, treatment, complications, prevention. arthritis, arthrosis temporomandibular joint (TMJ): classification, clinical course, diagnosis, treatment, complications and prevention. TMJ syndrome of pain disfunction. Surgical TMJ arthroscopy.
CLINICAL SYMPTOMS ACUTE SINUSITIS < 3 weeks SUBACUTE SINUSITIS 3 weeks-3 months CHRONIC SINUSITIS > 3 months
SYMPTOMS Bloked nose Headache Fever Yellow or green-coloured mucus from the nose Swelling of the face Aching teeth in the upper jaw Loss of the senses of smell and taste Persistent cough Generally feeling unwell
MAXILLARY SINUSITIS FROM DENTAL ORIGIN 1.Periapical abscess 2.Periodontal diseases 3.Infected dental cyst 4.Dental material in antrum 5.Oroantral communication
1.Periapical abscess Acute sinusitis Anaerobic organisms 2.Periodontal diseases Lane & O’Neal Chronic sinusitis 5 years irrigation + antibiotics examination communication with the maxillary sinus via a periodontal pocket
3.Infected dental cyst Periapical cyst Most common of all cysts of the oral region Epithelium rest of Malassez The cyst enlarges in to the maxillary sinus
4.Dental material in antrum 1.Displacement of root extraction third molar > second molar > canine Pa or occlusal film loss of lamina dura 2.Implant 3.Root canal overfilling
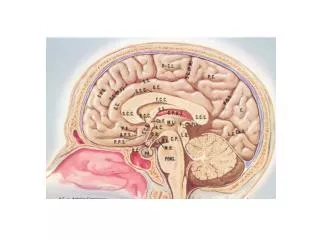
Normal Anatomy Mandibularcondyle (head) Glenoidfossa Articular tubercle (eminence)
Posterior band of articular disc Anterior band of articular disc Mandibular condyle (head) Lateral pterygoid muscle raphe Lower head of lateral pterygoid muscle Posterior disc attachment
Mandibular condyle (head) Articular disc
MRI and autopsy sections: upper row oblique sagittal MRI, asymptomatic volunteer: left lateral, middle medial, right opened mouth
Partial anterior disc displacement at baseline lateral sections central sections open-mouth
Complete anterior disc displacement medial section Autopsy Open-mouth MRI
Medial disc displacement coronal MRI Oblique coronal MRI
Osteoarthritis Definition • Non-inflammatory focal degenerative disorder of synovial joints, primarily affecting articular cartilage and sub-condylar bone; initiated by deterioration of articular soft-tissue cover and exposure of bone. Clinical Features • Crepitation sounds from joint(s) • Restricted or normal mouth opening capacity • Pain or no pain from joint areas and/or of mastication muscles • Occasionally, joints may show inflammatory signs • Women more frequent than men
anteriorly displaced and deformed, degenerated disc and irregular cortical outline with osteophytosis and sclerosis of condyle .
Advanced osteoarthritis and anterior disc displacement, with joint effusion
Imaging Features • Abnormal signal on T2-weighted image from • condyle marrow: increased signal indicates marrow edema; reduced signal indicates marrow sclerosis or fibrosis • Combination of marrow edema signal and marrow sclerosis signal in condyle most reliable sign for histologic diagnosis of osteonecrosis • Marrow sclerosis signal may indicate advanced • osteoarthritis without osteonecrosis, or osteonecrosis
Arthritides Definition • Inflammation of synovial membrane characterized by edema, cellular accumulation, and synovial proliferation (villous formation). Clinical Features • Swelling of joint area, not frequently seen in TMJ • Pain (in active disease) from joints • Restricted mouth opening capacity • Morning stiffness, in particular stiff neck • Dental occlusion problems; “my bite doesn’t fit” • Crepitation due to secondary osteoarthritis
Rheumatoid arthritis. After 1 year
Rheumatoid arthritis. A MRI shows completely destroyed disc, replaced by fibrous or vascular pannus and cortical punched-out erosion (arrow) with sclerosis in condyle.
Psoriatic arthropathy. Obliquecoronal and oblique sagittal CT images show punched-out erosion in lateral part of condyle (arrow). Psoriatic arthropathy. MRI shows contrast enhancement within bone erosion and in joint space, consistent with thickened synovium/pannus formation. Openmouth MRI shows reduced condylar translation but normally located disc (and normal bone in this section)
Ankyloses Definition Fibrous or bony union between joint components.
Growth Disturbances (Anomalies) Definition Abnormal growth of mandibular condyle; overgrowth, undergrowth, or bifid appearance.
Condylar hypoplasia and facial asymmetry Condylar Hypoplasia Normal TMJ
Inflammatory or Tumor-like Conditions Calcium Pyrophosphate Dehydrate Crystal Deposition Disease (Pseudogout)
Benign Tumors Synovial Chondromatosis • Benign tumor characterized by cartilaginous metaplasia of synovial membrane, usually in knee, producing small nodules of cartilage, which essentially separate from membrane to become loose bodies that may ossify.
Temporomandibular Disorders(TMDs) • Different pathologies affecting the masticatory muscles, the temporomandibular joint (TMJ), and related structures • Affects more than 25% of the population • 90% of those seeking treatment are women
Facial pains/Muscle spasms Pain/tenderness in the muscles of mastication and joint Joint sounds (popping, clicking) Limited jaw motion Jaw locking open or closed Headaches Teeth grinding Abnormal swallowing Uncomfortable “off” bite Inability to comfortably open/close mouth Dizziness/vertigo Ringing in the ears Visual disturbances Insomnia Tingling in hands/fingers Deviation of jaw to one side Signs/Symptoms
TMJ Anatomy • Osseous Anatomy • The articulation between the condyles of the mandible and the temporal bone, which is part of the cranium. • The articular surface of the condyle is convex and the articular eminence of the temporal bone is concave.
TMD Treatment • Working together: • Dentists • Orthodontists • Psychologists • Physical Therapists • Ear, Nose, Throat Doctor • Physicians • Alternative Medicine
TMD Examination • MRI • X-Ray • Dental examination for bite alignment
Physical Therapy Treatment • Physical Therapy is an important aspect in the treatment for TMD to: • Relieve musculoskeletal pain • Decrease inflammation • Restore normal joint/muscular movements for oral motor function • Correct poor posture
TMJ Evaluation • History • Posture • Watch, feel, listen to jaw with AROM • Opening between 40-50mm • Protrusion/retraction between 8-10mm • Lateral deviation while opening (S or C curve) • Lateral excursion 8-10mm • Ligamentous Laxity testing • Transverse Ligament • Alar Ligament • Cervical ROM testing • Palpate joints/muscles for tenderness
Therapeutic Exercises Manual Therapy Modalities Electromyographic (EMG) Biofeedback Dental Splint Types of Treatment
Improve muscular coordination Increase muscular strength Postural exercises Active ROM exercises Muscles of mastication Cervical spine muscles General mobility Therapeutic Exercise
Make a “clicking” sound with the tongue on the roof of the mouth. This slightly opens the jaw with the tongue on the palate behind the front teeth, which is the resting position of the jaw and the first portion of relaxation exercises. Place tip of tongue on palate behind teeth and draw small circles. Place tip of tongue on hard palate and blow air out, rolling the tongue, or making a “r r r r” sound. Techniques: Tongue Proprioception and Control
Techniques: Control ofJaw Muscles • Begin with proper resting position of the jaw. Teach the patient control while elevating and depressing the mandible throughout the first half of the ROM. • Keeping the tongue on the roof of the mouth, the patient opens the mouth while trying to keep the chin in midline. Use a mirror for visual reinforcement. • If the jaw deviates to one side, teach the patient to practice lateral deviation to the opposite side without creating pain or excessive motion.
Long Axis Distraction: Sitting/Supine PT positioned opposite of affected side Use hand opposite of affected jt. side Thumb in mouth on last molar Apply gentle downward pressure with thumb Hold for ~30 seconds 2-3x/session Bilaterally Anterior Glide Same hand placement Slightly distract using DIP of thumb while gliding anteriorly Oscillate for 30 seconds Joint Mobilizations