Download
1 / 54
540 likes | 690 Views
Knee Anatomy. Reza Omid, M.D. Assistant Professor Orthopaedic Surgery Shoulder & Elbow Reconstruction Sports Medicine Keck School of Medicine of USC. Bony Anatomy. Tibiofemoral joint Patellofemoral joint. Femoral Condyles. A – Lateral Condyle Smaller radius of curvature

E N D
Knee Anatomy Reza Omid, M.D. Assistant Professor Orthopaedic Surgery Shoulder & Elbow Reconstruction Sports Medicine Keck School of Medicine of USC
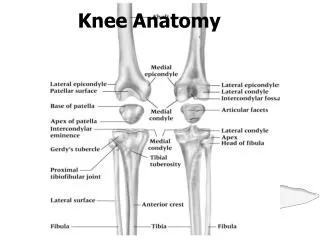
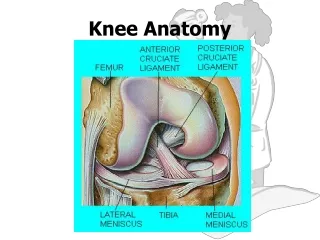
Bony Anatomy • Tibiofemoral joint • Patellofemoral joint
Femoral Condyles • A – Lateral Condyle • Smaller radius of curvature • Smaller in all dimensions • Extends more anteriorly • B – Medial Condyle • Larger radius of curvature • Extends more distally • C – Intercondylar notch
Tibial Plateau • D – Medial Plateau • Greater surface area • Concave • Circular shape • E – Intercondylar Eminence • F – Lateral Plateau • Smaller surface area • Convex • Oval shape
Patella • Sesamoid bone in quadriceps • Dividing central ridge • Comprised of seven facets • Medial and Lateral facets divided into 3rds • 7th facet is most medial (odd facet) • Medial half usually smaller • Thick hyaline cartilage (5.5mm)
Femoral Sulcus • Lateral wider and higher • Both with sagittal convexity
Screw Home Mechanism • Knee achieves terminal extension via the “screw home mechanism • The tibia externally rotates in relation to the femur. • When the knee needs to flex, the popliteus contracts which causes internal rotation of the tibia and in essence unlocking the knee and allowing it to bend
Popliteal Artery • Originates at the adductor hiatus and passes through the popliteal fossa, then deep to the fibrous arch over the soleus muscle • Divides into the anterior and posterior tibial arteries at the distal aspect of the popliteus muscle
Popliteal Artery • The popliteal artery is 9mm posterior to the posterior cortex of the tibia at 90° of flexion and even closer in extension. • Place retractors biased to the medial side when possible.
Skin Blood Flow • If two longitudinal incisions are present, the more lateral incision should be used (if allows adequate exposure) because most of blood supply comes in medially. • The lateral skin edge is more hypoxic than the medial skin edge so keep this in mind when placing sutures.
Tibial Nerve • Initially lateral to the popliteal artery • Crosses at midpoint to end medial to the artery at soleus arch
Common Peroneal Nerve • Lateral aspect of the popliteal space • Medial and posterior to the biceps femoris tendon
Patellofemoral Biomechanics • Joint Reactive Force • In flexion, patella compressed onto femur creating joint reactive force • Stair climbing – 3.5 X BW • Deep bends – 7-8 X BW
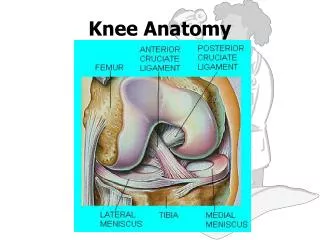
Menisci • Primarily type I collagen with fibers arranged obliquely, radially, and vertically • Outer 10% to 30% has blood supplied from the perimeniscal capillary plexus off the superior and inferior medial and lateral genicular arteries
Meniscus Function • Load Transmission • 50% load transmitted in extension • 85% load transmitted at 90 degrees flexion • Resection of 15-34% increases pressure 350% • Secondary Stabilization • Medial meniscus provides anterior restraint • Especially in ACL deficient knee
Lateral Meniscus • Loose peripheral attachment allows greater translation during motion • Average excursions of the menisci with knee flexion • 5.2 mm for the medial • 11 mm for the lateral • Bare area anterior to popliteus tendon • Two highly variable meniscofemoral ligaments attach it to medial femoral condyle: • Anterior – Humphrey • Posterior – Wrisberg’s
Ligaments • Tensile strengths of various knee ligaments: • MCL ~ 4400-5000N • PCL ~2500-3000N • ACL ~ 2200-2500N • LCL ~750N
Anterior Cruciate Ligament • 26-38 (33) mm in length • ACL graft selection you aim for at least 100-110mm graft length because it needs about ~33mm for the tibial tunnel, ~33mm for the femoral tunnel and ~33 for the graft itself • 11 mm in width • Primary restraint • Anterior translation of tibia (74-85%) • Normal 3-5mm of translation • Secondary restraint • Internal rotation • Varus/Valgus • Hyperextension
Anterior Cruciate Ligament • Two bands • Anteromedial band taut in flexion • Posterolateral band taut in extension
Anterior Cruciate Ligament • Femoral Attachment • Posterior portion of medial surface of LFC • Oriented in line of axis of femur in extension • Footprint in shape of circular segment • Posterior convexity 4 mm anterior to articular surface • Surface area measures 16-24 x 11 mm • Lateral to midline on AP view • Posterosuperior on lateral view
Anterior Cruciate Ligament • Tibial Attachment • Anterolateral to medial spine • Insertion has oval shape • Sections attach to bone, AHLM, PHLM • 15 mm posterior to anterior tibia • 17-30 x 11 mm surface area • Just lateral to midline on AP • 40% back on lateral view
Lateral Bifurcate Ridge • Running perpendicular to the lateral intercondylar ridge) seperates the origins of the anteromedial and posterolaterla bundles.
Lateral Intercondylear Ridge • Resident’s ridge on the lateral femoral condylar wall denotes the lateral intercondylear ridge and marks the most anterior and superior extent of the femoral origins of the ACL.
Anterior Cruciate Ligament • Blood Supply • ACL completely ensheathed in fold of synovial membrane • Although intraarticular, technically extrasynovial • Main supply is middle geniculate with smaller contribution from both inferior geniculates • Innervation • Branches of tibial nerve • Very few pain receptors in substance of ACL
Posterior Cruciate Ligament • 38 mm in length • 13 mm in width • Narrowest diameter at midsubstance • Anterolateral band • More robust, Taut in flexion • Posteromedial band • Thinner, Taut in extension
Posterior Cruciate Ligament • Femoral Attachment • Lateral surface MFC • Shape of circular segment • Distal margin 3 mm proximal to articular surface
Posterior Cruciate Ligament • Tibial Attachment • Depression between tibial plateaus • 1 cm distal to tibial articular surface • Can have contributions to PHLM as well as meniscofemoral ligaments • Average width 13 mm
PCL Biomechanics • Function • Primary restraint • Posterior translation of tibia (90-95%) • Greatest translation occurs at 75 degrees flexion • Secondary restraint • Varus/valgus • External rotation
Medial Structures • Layer 1: Deep fascia and Sartorius • Layer 2: Superficial MCL, MPFL • Layer 3: Joint capsule, Deep MCL
Medial Ligaments • Superficial MCL (Medial Collateral Ligament) • Originates on medial epicondyle • avg: 3.2 mm proximal and 4.8 mm posterior to medial epicondyle • Tibial insertions (2) distal and proximal • Proximal: anterior arm of the semimembranosus tendon • Distal: broad-based, just anterior to the posteromedial crest of the tibia, most located within the pesanserine bursa • Posterior Oblique Ligament (POL) • superficial, central (main component), and capsular arms • Deep MCL • Divided into meniscofemoral and meniscotibial ligaments
MCL Biomechanics • Stability – Most important in flexion when posterior structures relaxed • Valgus rotation • External rotation • Medial/Lateral translation • Superficial MCL most important for stability (57-78%) • Sectioning Deep MCL does not result in instability if Superficial MCL intact
Medial Patellofemoral Ligament • Runs transversely in Layer 2 • Originates from adductor tubercle, femoral epicondyle, and superficial MCL • Proximal fiber inserts on undersurface of VMO and vastusintermedius • Distal fibers insert on superomedial patella • Width averages 1.3 cm
MPFL Biomechanics • Soft tissue restraint of extensor mechanism • Patella subluxes most easily at 20° knee flexion • MPFL resists patellar lateral subluxation greatest in extension • Primary stabilizer followed by patellomeniscal, patellotibial, and medial retinaculum
Lateral Structures • Layer 1 • IT band • biceps tendon • Layer 2 • Lateral retinaculum • patellofemoral ligaments • Layer 3 • Joint capsule • LCL • arcuate ligament • fabellofibular ligament • popliteofibular ligament
Lateral Structures • Layer 1 • IT band • biceps tendon • Layer 2 • Lateral retinaculum • patellofemoral ligaments • Layer 3 • Joint capsule • LCL • arcuate ligament • fabellofibular ligament • popliteofibular ligament
Iliotibial Band • Coalescence at greater trochanter of tensor fascia lata, gluteus medius and gluteus maximus • IT band continues distally to form the: • IT tract • Inserts distally on Gerdy’s tubercle and on distal femur through intermuscular septum • Iliopatellar band • Inserts on lateral patella resisting medial directed forces
IT Band Biomechanics • Functions • Stabilizes against varus opening • Knee extensor in extension • Knee flexor in flexion • External rotator of tibia in >40 flexion
Lateral Collateral Ligament • Arises in fovea slightly proximal (1.4 mm) and posterior (3.1 mm) to lateral epicondyle • Attaches to V-shaped plateau of fibular head (8.2mm distal to anterior edge) • Surrounded by biceps femoris tendon distally • Average length 59-71 mm • AP diameter 3.4 mm ML diameter 2.3 mm
LCL Origin • Posterior (4.6 mm) and proximal (1.3 mm) to the lateral femoral epicondyle • Posterior and superior to the insertion of the poplitieus (18mm away from each other)
LCL Biomechanics • Tightest in extension, 0-30 degrees • Becomes looser in flexion >30 degrees • Primary restraint to varus • Secondary restraint to ER and posterior translation
Posterolateral Corner • FCL • Popliteus tendon • Popliteofibular lig
Posterolateral Corner • Static Stabilizers (highly variable) • LCL • Fabellofibular ligament • Short lateral ligament • Popliteofibular ligament • Arcuate ligament • Posterolateral capsule • Posterior horn lateral meniscus • Lateral coronary ligament
Posterolateral Corner • Dynamic Stabilizers • IT band • Lateral gastrocnemius • Biceps femoris • Popliteus
Popliteus Complex • Dynamic • Popliteus muscle • Static • Popliteofibular ligament • Popliteotibial fascicle • Popliteomeniscal fascicle