Download
1 / 86
900 likes | 1.37k Views
Nematode I. Main contents of last time. Parasite / parasitology / parasitism terms of Parasitology Relationship of parasite and it’s host Classes of parasites Classes of hosts Epidemiology and control of parasitic diseases Characteristics of Class Nematoda.

E N D
Main contents of last time • Parasite / parasitology / parasitism • terms of Parasitology • Relationship of parasite and it’s host • Classes of parasites • Classes of hosts • Epidemiology and control of parasitic diseases • Characteristics of Class Nematoda
According to the biological classification-- The helminths of medical importance belong to 3 classes: Nematoda Trematoda Cestoda
According to the type of life cycle: • Geohelminths • Biohelminths
About the nomenclature of parasite • Each parasite possesses two names, a generic and a specific; • The former begins with an initial capital and the latter with an initial small letter; • After which comes the designator’s name; • Followed by punctuation and finally the year; • The generic and specific name are in italics.
Class Lobosea • Class Zoomastigophorea • Class Sporozoa • Class Ciliophora Medical Protozoology Human Parasitology • Class Nematoda • Class Trematoda • Class Cestoda • Class Metacanthocephala Medical Helminthology • Class Insecta • Class Arachnida • Class Crustacea • Class Chilopoda Medical Arthropodology
Nematode: molt 4 times in the larva stage Example: Butterfly Larva shedding skin (Just an example but not nematode!)
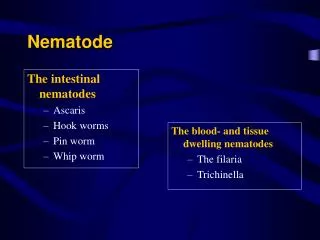
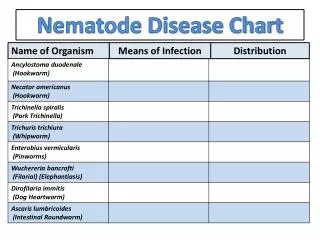
Nematode I A.Trichinella spiralis (The trichina worm) B. Trichuris trichiura( Whipworm) C. Capillaria philippinensis D. Strongyloides stercoralis E. Hookworms
Trichinella spiralis(p161) Biohelminth. Members of the genus Trichinella are able to infect a broad spectrum of mammalian hosts, making them one of the world’s most widely-distributed group of nematode infections.
Morphology 1.Adult: Small and slender. • male: 1.4~1.8mm x 36 µm; with two lobed appendages called alae. • Female: 1.4~4mm x 36 µm; with formed larvae in uterus.
Adult female T. spiralis. 3 mm x 36 µm. Note fully formed larvae in uterus Adult male T. spiralis. Note claspers on tail (lower end). 1.5mm x 36 µm
2. Larva a. newborn larva:70 x 7 um; b. encapsulated larva: Nurse cell-parasite complex.Spiral shaped, residing in the striated muscles of the host, and is enveloped by a double, ellipsoidal capsule(0.25- 0.5x0.21-0.42mm; larva: 1mm)
Encapsulated larva Encapsulated larva Encapsulated larva Encapsulated larva Encapsulated larva Encapsulated larva Encapsulated larva Encapsulated larva
Encapsulated larva: Nurse cell-parasite complex Newborn larva of T. spiralis. 0.08 mm long by 7 µm in diameter
Life cycle • Infection is initiated by ingesting raw or undercooked meats harboring the Nurse cell-larva complex. • Larvae are released from muscle tissue by digestive enzymes in the stomach, and then locate to the upper two-thirds of the small intestine.
Life cycle • The outermost cuticular layer (epicuticle) becomes partially digested. This enables the parasite to receive environmental cues and to then select an infection site within the small intestine. • The immature parasites penetrate the columnar epithelium at the base of the villus.
Life cycle • Larvae molt four times in rapid succession over a 30-hour period, developing into adults. • After mating, adult females produce live offspring — newborn larvae— which measure 0.08 mm long by 7 µm in diameter.
Life cycle • Expulsion of adult worms from the host is the final expression of immunity, and may take several weeks. • Most newborn larvae enter the general circulation, and become distributed throughout the body.
Migrating newborns leave capillaries and enter cells. There appears to be no tropism for any particular cell type. • Once inside, they can either remain or leave, depending upon environmental cues received by the parasite. • Most cell types die as the result of invasion. Skeletal muscle cells are the only exception.
Not only do the parasites remain inside them after invasion, they induce a remarkable series of changes, causing the fully differentiated muscle cell to transform into one that supports the growth and development of the larva. This process is termed Nurse cell formation.
Immunology • The infection induces two types of immunity: cellular and humoral immunity. • Cell-mediated immunity: eliminate the adult worms. • Humoral antibodies developing in the course of infection: are not protective but can be used for diagnosis. • IgE fraction of serum gamma globulin is greatly increased.
Pathogenesis and clinical Manifestation Adult worm and both migratory and encysted larvae are pathogenic: • Adult female worms present in the intestine cause gastrointestinal disturbances; • Migrating larvae cause various allergic manifestation such as fever, edema of the face, eosinophilia, and • Encysted larvae in the skeletal muscles cause muscular pain.
The process of pathological change: three phases a)Invade phaseThe phase occur within the first week after ingestion of infected meat, during the intestinal phase; this phase is associated with the development of larvae develop into adult. For invading of larvae and adult worms, the wall of intestine is damaged.
Microscopic ulceration, mucosal hyperemia, localized edema, punctate hemorrhages, and intestinal inflammation may main pathological changes. Gastrointestinal signs and symptoms may be the first evidence of infection, including fever, disgusting, vomiting, abdominal discomfort, diarrhea etc.
b) Migratory phaseThis phase, beginning about 7 to 9 days after exposure, is associated with penetration of the newborn larvae into muscle cells, initiating a strong inflammatory response. Later, the fibers enlarge, and edema, nuclear proliferation, and intestinal inflammation ensue, and fibrosis.
Early symptoms of this stage are: - Swelling of the eyelids and facial edema. - Following this, muscle swelling, tenderness, pain on movement, and fever usually develop.
- Within the first two weeks of severe systemic disease, allergic phenomena such as edema, pneumonitis, and pleural transudate may occur. - Serious complications, including myocarditis, and meningoencephalitis, occur most often in the third to ninth week of the disease.
c) Encystation of the larvae and tissue repair The formation of cyst result in the stimulation of larvae and tissue reparation. With encystation, the inflammation disappear gradually, the clinical manifestation become light, but the muscular pain can still last for months.
Diagnosis • Parasitic diagnosis; • Immunodiagnosis .
Definitive diagnosis depends upon: - finding the Nurse cell-parasite complex (encysted larva) in muscle biopsy by microscopic examination or - detection of Trichinella–specific DNA by PCR. PCR is very sensitive and specific for detecting small numbers of larvae in muscle tissue, but for some reasons it’s not routine method till now.
Muscle biopsy can be negative, even in the heaviest of infections, due to sampling errors. In addition, the larvae may be at an early stage of their development, making them inconspicuous, even to experienced pathologists. • Immunodiagnosis a) Interdermal test (IDT) for screening in population; b) Detecting for antibodies such as ELISA etc.
Treatment Mebendazole given early during the infection may help reduce the number of larvae that might lead to further clinical complications, but it’s difficult to make diagnosis early. Anti-inflammatory corticosteroids, particularly prednisolone, are recommended if the diagnosis is secure.
Rapidly destroying larvae with anthelminthics without use of steroids may actually exacerbate host inflammatory responses and worsen disease.
The myopathic phase is treated in conjunction with antipyretics and analgesics (aspirin, acetaminophen), and should be continued until the fever and allergic signs recede. Because of their immunosuppressive potential, steroids should be administered with caution.
Epidemiology • Human and animal infections of T.spiralis is worldwide distribution. • Eating or ingesting raw pork with larva cyst is major route to infection. • The cyst have strong resistance to low temperature, freezing at -15℃ for 20 days can destroy the parasites in the pork. Cyst can be killed at 70℃, so eating non-properly processed meat products is the way to be infected.
Prevention and Control • Regular inspection of meat, avoidance of eating raw or undercooked pork and meat of other wild animals; and avoidance of feeding raw garbage to pigs will prevent transmission of infection to man.
Treatment of the immature worms in the small intestine is usually successful and will abort or markedly inhibit systemic disease, so treatment of the intestinal phase in all cases up to six weeks after infection is advisable. Albendazole is the effective drug for trichinellosis. Mebendazole is also recommended, it is believe to kill both adult worms and larvae.
Trichuris trichiura ( Whipworm) • Geohelminth • Worldwide • (p164)
I. Morphology: • Adult:Adult worms characteristically are whip-shaped, the anterior three-fifth being long, thin and hair-like and the posterior one-to-two fifth being short, thick and stout. Males are slightly smaller than females, the latter measuring 35~50 mm in length.
In both sexes, a capillary-like esophagus extends two-thirds of the body length and is encircled along much of its length by a series of unicellular glands. The cells can excrete some enzymes which possess antigenicity.
Egg:The egg is typically barrel-shaped with two polar plugs. These are yellowish brown and double shelled. The eggs measure 50~54×22~23μm . The eggs contain an unsegmented ovum each, when passed in the faeces. These freshly passed eggs are not infective to humans.
II. Life Cycle 1. Site of inhabitation: cecum 2. Infective stage: embryonic egg 3. Infective mode and route: passively swallowed by the mouth 4. Without intermediate host and reservoir host 5. The life span of the adult is about 3-5years. deposit 3weeks ingested by man Adults Eggs Infective eggs larvae hatch out in small intestine invade the intestinal wall return to the intestinal lumen Adults develop 3-10 days