Download
1 / 53
540 likes | 694 Views
Will Blandamer. Director, GM Public Health Network “Public Health Priorities and Actions for Greater Manchester†GMCVO Workshop 20 th January 2011. Contents. Context – New Public Health System Local Public Health Arrangements Outcomes and Indicators Proposed

E N D
Will Blandamer Director, GM Public Health Network “Public Health Priorities and Actions for Greater Manchester” GMCVO Workshop 20th January 2011
Contents • Context – New Public Health System • Local Public Health Arrangements • Outcomes and Indicators Proposed • Population Health in Greater Manchester • GM Public Health Network - Priorities and Actions
Contents • Context – New Public Health System • Local Public Health Arrangements • Outcomes and Indicators Proposed • Population Health in Greater Manchester • GM Public Health Network - Priorities and Actions
“Healthy People Healthy Lives – A Public Health Strategy for England” Commitment to • protecting the population from serious health threats; • helping people live longer, healthier and more fulfilling lives; • improving the health of the poorest, fastest. • Life course opportunities to improve health
The White Paper is also a formal response to the review by Sir Michael Marmot of inequalities in health. The Paper should be seen in the wider context of the NHS, and Social Care White Papers respectively, with which it has considerable resonance Policy Linkages
Strategic Drivers 1 – Marmot Review The recent Marmot Review Fair Society, Healthy Lives (DH, 2010) identifies 6 key policy areas to tackle Health Inequalities and priority actions: • Give every child the best start in life • Enable all children, young people and adults to maximise their capabilities and have control over their lives • Create fair employment and good work for all • Ensure healthy standard of living for all • Create and develop healthy and sustainable places and communities • Strengthen the role and impact of ill health prevention
The Boorman Review, NHS Health and Wellbeing 2009, sets out ways in which staff satisfaction could be improved Implementing the review could save the NHS up to £555 million nationally Focuses on prevention and health improvement, providing efficient support for staff who present with ill health, being proactive in tackling the causes of ill health (both work and lifestyle related) and, where there are clear benefits, providing early intervention services Implementation of the Boorman Review is a priority in the NHS Operating Framework for 2010/11. Trusts will be assessed on it by the Care Quality Commission Strategic Drivers 2 – Boorman Review
Further Policy • During 2011, the Department of Health will publish documents that build on this new approach, on mental health, tobacco control, obesity, sexual health, pandemic flu preparedness, health protection and emergency preparedness. • Workforce strategy by Autumn 2011
The Approach of Healthy People Healthy Lives reach across and reach out. responsive – owned by communities and shaped by their needs; resourced – with ring-fenced funding and incentives to improve; rigorous – professionally-led, focused on evidence, efficient and effective; resilient – strengthening protection against current and future threats to health
Key Developments 1 Local Authorities – strategic leaders for health & wellbeing – Joint Health & Well-being Strategy Statutory Health & Well-being Boards Public Health England (NTA,HPA, SHA, other PH) DPH joint appointment with enhanced powers in all upper tier authorities JSNA – an obligation on all commissioners Ring-fenced national PH budget - LAs plus central (shadow budgets during 2012-13)
Key Developments 2 New Health Premium New National Institute for Health Research (NIHR) School for Public Health Research and a Policy Research Unit on Behaviour and Health. Public health will be part of the NHS Commissioning Board’s (NHSCB)mandate. CMOwill lead a professional network for all those responsible for commissioning or providing public health.
The Director of Public Health • Will be the principal adviser on all health matters to the local authority, its elected members and officers, on the full range of local authority functions and their impact on the health of the local population • Will be play a key role in the proposed new functions of local authorities in promoting integrated working • Contribute to the development of the local joint strategic needs assessment (JSNA) and the joint health and wellbeing strategy • Be an advocate for the public’s health within the community • Produce an authoritative independent annual report on the health of their local population
Contents • Context – New Public Health System • Local Public Health Arrangements • Outcomes and Indicators Proposed 4. Population Health in Greater Manchester 5. GM Public Health Network - Priorities and Actions
1. Director of Public Health • Key member of health and well being board • Lead development of JSNA • Ensure high quality public health advice is available to commissioners • Advocate for the publics health within the community • Report on the health of their local population
2. Health and Well Being Board • Restoring democratic accountability for health • Ensuring all partners deliver their organisations commitment • Point of intersection between • Public health • Social care • Children's health and well being • NHS Commissioning • Joint NHS Commissioning
3. Public Health England • Local health and well being boards supported by “power and efficiency” of PHE • Supported by the joint appointment • Particular link on health protection • Allocation of ring fenced budget
4. Supra local networks • Economies of scale in supporting local function • Emergency planning, tobacco control, education and training, intelligence and evidence gathering • Sharing knowledge/enhancing capacity • Engagement with PHE and NCB
5. New approach to public health policy • “creating the conditions where people can take responsibility for their own health and well being” • Instead of focusing on deficits problems and needs this new approach will build on the assets of individuals families and communities and strengthen civic society
6. Effective intelligence and research • JSNA • Evidence of effective and cost effective programmes/interventions • Modelling to demonstrate impact of interventions • Surveillance and monitoring of hazards • Health Impact Assessment and Health Equity Audit
7. Workforce • Public Health professionalism • Public Health capacity building across sectors • Unlock the potential of voluntary, business, GP consortia and others to define outcomes and deliver interventions
8. Commissioning and Business Planning • Commissioning of Public Health Programmes – effective and proven –evidence of ROI • Engagement with NHS Commissioning Board re screening • Working with GP consortia (e.g. uptake for screening)
9. Health Protection • Local Authorities will need to ensure that they have access to sufficient resources and professional expert advice through their DPH to fulfil their statutory duties on health protection as part of civil contingencies planning and response, including • Major incidents • Infectious disease outbreaks • Port health
10. Health Improvement and Population Well being • Transfer of public health leadership back to local authorities allows focus and ownership of causes of inequality –”systematic scaled up and sustainable impact” • Damaging health behaviour – smoking, alcohol harm, nutrition • Socio-economic determinants – finding work, managing debt, early years, school, transport and housing
11. Population HealthCare • Joint commissioning of population health services -screening, immunisation, drug and alcohol services, sexual health services • Services for potentially excluded groups – homeless, prisoners and offenders, travellers • Equitable access to services • Support to clinical pathway redesign in line with JSNA priorities • Heath services accepting responsibility for health protection, emergency planning etc
Contents • Context – New Public Health System • Local Public Health Arrangements • Outcomes and Indicators Proposed • Population Health in Greater Manchester • GM Public Health Network - Priorities and Actions
Domain 1: Health Protection and Resilience The activities to deliver this domain can most appropriately be coordinated nationally by Public Health England and local authorities will contribute to these outcomes particularly in their role in leading local resilience arrangements and in providing surveillance information. Proposed indicators: • Comprehensive, agreed, inter-agency plans for a proportionate response to public health incidents are in place and assured to an agreed standard. • Systems in place to ensure effective and adequate surveillance of health protection risks and hazards. • Life years lost from air pollution as measured by fine particulate matter. • Population vaccination coverage (for each of the national vaccination programmes across the life course). • Treatment completion rates for TB. • Public sector organisations with a board approved sustainable development management plan.
Domain 2: Tackling the Wider Determinants of Ill Health Locally, Health and Wellbeing Boards will take a broad approach to health improvement requiring the full participation by all partners to focus on improving the wider determinants of health that drive poor health outcomes especially in the most disadvantaged. Proposed Indicators: • Children in poverty; • School readiness; • Housing overcrowding rates; • Truancy rates; • Incidents of domestic abuse; • Statutory homeless households; • Fuel poverty; • Access and utilisation of green space; • Reduction in proven re-offending; • Social connectedness; • Cycling participation; • Rates of violent crime; • First time entrants to the youth justice system; • Rates of adolescents not in education, training or employment; • Proportion of people with mental illness and/or disability in settled accommodation and/or in employment; • Proportion of people in long term unemployment; • Employment of people with long term conditions; • Killed or seriously injured casualties on England’s roads; • The percentage of the population affected by environmental, neighbour and neighbourhood noise; • Older people’s perception of community safety.
Domain 3: Health Improvement Helping people to live healthy lifestyles and make healthy choices) Nationally, there is a clear role for Government in contributing to delivering these indicators – through legislation or regulation, through partnerships with business and industry, through national campaigns. However, much of the delivery will take place at the local level – led by the Director of Public Health in partnership with Health and Wellbeing Boards, using the ring-fenced public health budget. Proposed Indicators: • Prevalence of healthy weight in 4-5 and 10-11 year olds; • Prevalence of healthy weight in adults; • Smoking prevalence in adults; • Rate of hospital admissions for alcohol related harm; • % of adults meeting recommended guidelines on physical activity; • Hospital admissions caused by unintentional and deliberate injuries to 5-18 year olds; • Number leaving drug treatment free of drug dependence; • Under 18 conception rate; • Rate of dental caries in children aged 5 years; • Self-reported wellbeing.
Domain 4: Prevention of Ill Health Nationally, the role of Government (in partnership with business and industry) will be critical. Across local Health and Wellbeing Partnerships, public health would share responsibility with the NHS, adult social care and children’s services. Proposed Indicators: • Prevalence of recorded diabetes; • Work sickness absence rate; • Screening uptake; • Chlamydia diagnosis rates; • Child development at 2 - 2.5yrs; • Maternal smoking prevalence; • Hospital admissions caused by unintentional and deliberate injuries to under 5s; • Rate of hospital admissions as a result of self harm; • Incidence of low-birth weight of term babies; • Breastfeeding initiation and prevalence at 6 - 8 weeks after birth; • Proportion of persons presenting with HIV at a late stage of infection; • Smoking rate of people with serious mental illness; • Emergency readmissions rates to hospitals within 28 days of discharge; • Health related quality of life for older people; • Acute admissions as a result of falls or fall injuries for over 65s; • Take up of NHS Health Check programme by those eligible; • Patients with cancer diagnosed at Stage 1 and 2 as a proportion of cancers diagnosed.
Domain 5: Prevention of premature mortality At the local level, improvements in these indicators will be driven by local Health and Wellbeing Partnerships with shared responsibility across the NHS, public health and care services. Some delivery will be for other local partners to prevent seasonal mortality, National contribution across Government, the NHS Commissioning Board and other national bodies in setting policy or to avoid mortality as a result of major emergencies. Proposed Indicators: • Infant mortality rate; • Suicide rate; • Excess seasonal mortality; • Mortality rate of people with mental illness; • Mortality rates from the following diseases in the u75s: communicable disease; cardiovascular disease; cancer; chronic liver disease; chronic respiratory disease.
Contents • Context – New Public Health System • Local Public Health Arrangements • Outcomes and Indicators Proposed • Population Health in Greater Manchester • GM Public Health Network - Priorities and Actions
Contents • Context – New Public Health System • Local Public Health Arrangements • Outcomes and Indicators Proposed • Population Health in Greater Manchester • GM Public Health Network - Priorities and Actions
GM Leadership – An Audit Commission View “Greater Manchester knows what the health inequalities issues are –BUT There is no health vision for Greater Manchester and a lack of champions. Concerted, radical action is required to make a difference and reduce the health inequalities gap” Audit Commission May 2006
Achievement of target to reduce smoking in manual social groups:smoking cessation & tobacco control. Targeted smoking cessation at patients with CVD and COPD = 2% reduction in unplanned admissions within 1 year. Prevention and effective management of other risk factors in primary care e.g. high blood pressure, diabetes, weight management etc Targeting over-50s where the greatest short-term impact on life expectancy will be made through achievement of flu vaccination/pneumococcal targets. Evidence of active engagement with key local partners on issues affecting life expectancy -e.g. joint health social care investment plans, falls prevention in older people, tobacco control, school food. Brief focal interventions for alcohol misuse in Primary care. Establishing a pulmonary rehabilitation programme could result in a reduction of 26.3% respiratory readmissions and 44.8% bed days a year. Targeted primary care nurse –led heart failure management: up to 50% of readmissions of heart failure patients may be preventable Public Health – What Works locally and quickly and is in local gift
Collaborative Work on Public Health in GM - Projects • Public health underpinning of stroke service reconfiguration • Hepatitis C Strategy • Management of Screening Programmes • Leadership on Alcohol • Social Marketing and Promotional Activity • Cancer Inequalities Strategy • Cardiac Inequalities Strategy • GM Suicide Prevention Partnership • AAA Screening Implementation
More projects… • Gm Fuel Poverty Project • Collaborative implementation of health trainers • Pathway development for healthy weight services • Tobacco control joint working on promotion and prioritisation of illicit tobacco • Chlamydia Screening Programme • Media Partnerships – “iloveme” • Prioritisation of Domestic Violence • Salt Reduction
Creation of Capacity • Public Health Practice Unit • Arts and Health Network • GMCVO - capacity in voluntary sector • Close working with HPA • Regional Health Work and Well Being Programme • Regional Health and Migration Project • Regional A/N and N/B Screening programme
Partnerships – building influence • AGMA – Commissions • Commission for New Economy partic. • GMP • GM Fire and Rescue • GM Sport • GMPTE • Universities • Manchester – e.g. obesity atlas, suicide audit • Salford – e.g. Child health inequality • MMU – e.g. CPD development
GM Organisational Coherence The Architecture for Greater Manchester
Economic Coherence (Reference Manchester Independent Economic Review) • Most significant economic agglomeration outside London • A single functional economy • 2.5 million residents across 10 boroughs • 1.7 million working age population • £40 billion GVA annually (5% of UK GVA, 40% of North West) • 94,000 workplaces – 79,000 of which <10 employees • Local Economic Partnership
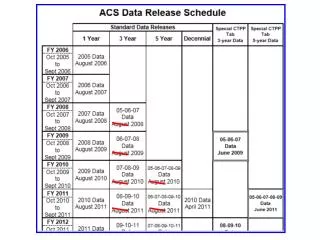
Pennine Acute GM – Acute Patient Flows (2007/08) PCT 3% Bury 66% 3% WWL Bolton 3% 53% 7% Acute ALW 6% 86% 11% 7% 3% 0.2% 5% 4% 4% 8% HMR 6% 7% 17% 4% 4% 2% MH 3% 75% 3% 5% Bolton 8% 4% Salford Oldham 18% BST MH 59% 0.01% 17% 52% 5% 13% 9% 3% Salford 4% 5% Pennine Care CMMC 19% 2% Stockport 3% Trafford T&G 0.01% 47% 16% 13% MCR 4% 3% 3% Christie 15% 47% 4% 14% 4% 51% MCR MH Trafford Tameside 5% 33% 6% 4% Stockport 2% 23% 11% UHSMFT 27% 14% 7% 11%
GM Leadership – An Audit Commission View “Greater Manchester knows what the health inequalities issues are –BUT There is no health vision for Greater Manchester and a lack of champions. Concerted, radical action is required to make a difference and reduce the health inequalities gap” Audit Commission May 2006 “There is much to be proud of. We outlined at that time what we hoped our report might look like in 2008. We can report with some confidence that this is now a good description of the position as it currently exists across Greater Manchester in 2008. This is a remarkable achievement in a short space of time.” Audit Commission October 2008
Current Focus of GM wide Partnership Work • GM Strategy Delivery • Work Programme Implementation • Support to Early Years prioritisation • Support to LTP3 • Submission of Local Sustainable Travel Fund • Promotion of Fuel Poverty agenda on Urban Retrofit • Informing GM Spatial Planning Framework • Support to “Changing Lives” – AGMA Sport and Physical Activity Strategy • GMP re Domestic Violence • Work across AGMA re Minimum Unit Pricing • Working with professional sports clubs • Working with Healthcare providers • Development of GM Health Commission role • Community Budget Implementation • Raised profile of tobacco control • Cancer Awareness Campaign Implementation • Promotion and Awareness of 20mph limits
GM wide public health functions • Focused on creation of added value locally – seeking collaborative advantage • Sharing expertise • Economies of Scale • Mechanism for influencing policy at GM level through Combined Authority etc • Engagement of organisations with GM spatial footprint • Securing GM as the lowest possible spatial level (e.g. National Commissioning Board) • Building where GM already has a national reputation for public health leadership • Support for a GM Health and Well Being Board?