Download
1 / 29
310 likes | 400 Views
Learn about aGVHD, its terms, symptoms, skin rash, liver and gut involvement, diagnosis via biopsy, staging, and more in this teaching session from July 2004 by Meg Browning. Dive into the historical perspective, technical details, and factors that create a GVHD setup.

E N D
Acute Graft Versus Host Disease(aGVHD) Teaching session 1 July, 2004 Meg Browning
Definition of terms • GVH(D): Graft-versus-host (disease). The set of symptoms that occur when the immune cells from a graft (marrow, organ, even transfusion) react against the recipient. • MHC: major histocompatibility complex; the primary proteins that identify “self.” We currently measure 10 genetic alleles for such proteins. These genes sort together, so you get them as sets from your parents, not as individual proteins. • Syngeneic: matching exactly (e.g., identical twins) • Allogeneic: not matching at some level (a “matched sibling” is still allogeneic!) • Autologous: (autogeneic, sadly, isn’t a word): from self
A brief note on “acute” and “chronic” • The classic definition is whether or not the patient is within the first 100 days after transplant; thus, “acute” GVH occurs before day 100. • There are pathological differences, as seen on biopsy, between disease states that would be considered chronic vs. acute • The red skin rash we see is acute; the chronic skin disease is more like scleroderma • Profuse watery diarrhea is consistent with acute; wasting is more chronic
Boring “historical perspective” slide • A fatal syndrome of skin abnormalities and diarrhea (or wasting, in newborns) given allogeneic spleen cells after irradiation (or in the newborns, at all). • Primary disease was the same thing after irradiation itself. • This was in the 1950’s, and in mice. Primary disease Secondary disease (GVHD)
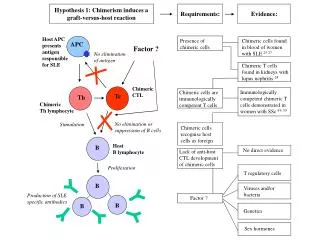
1966 (original, Billingham) definition • Criteria for the development of GVHD: • The graft must contain immunologically competent cells. • Still true • The host must possess alloantigens that are lacking in the graft (must appear foreign). • True in the parenthetical explanation • The host must be incapable of mounting an effective anti-graft reaction, at least for a period of time. • True as long as you emphasize “effective.”
Picky technical slide #2 graft IL-1 IFN TNF IL-2 foreign cell (non-self) The antigen-presenting cell recognizes a foreign cell, processes it, and presents antigen. The T cell is activated, leading to prolif- eration, cytokine production, etc.
Trick Question • Can recipients of autologous (and/or syngeneic) transplants still get GVHD? • Yes. • (OK, so it loses something when I warn you it’s a trick.) • How? • possibly thymic damage, and/or regulatory imbalance
alloreactivity degree of mismatch strength of mismatch sex mismatch donor parity age recipient age 20%, 30%, and 80% at <20, 45-50, and >50 donor age stem cell source cord: ?less marrow PBSC: more chronic whether T cell depleted microbes particularly herpes family conditioning immune suppression organ damage prophylaxis What creates a GVHD set-up?(or lack thereof)
Acute GVHD • Occurs within the 1st 100 days post-transplant; typically between days 4+ and 40. • Triad of dermatitis, enteritis, and hepatitis • ocular symptoms, pneumonitis, and hemorrhagic cystitis may also occur acutely, as may thrombocytopenia and anemia. • 40% of all HLA-matched recipients still get GVHD! • GVHD increases the risk of sepsis and certain other complications • aGVHD patients are more likely to have cGVHD • There is no racial or gender predilection • GVHD may decrease the likelihood of relapse
Skin is usually first • Red to violet lesions, often starting on palms and soles. May hurt or itch. Becomes confluent over cheeks, ears, neck, trunk; papules may form. In severe cases, bullae and epidermal necrosis occur. • DDx: scalded skin syndrome (infection), viral exanthem, chemo/radiation effects, drug allergy. • Biopsy or serial biopsies are helpful in Dx. • Biopsy findings are graded, not staged • Liver or GI involvement is unusual WITHOUT skin involvement
More skin GVH issues • Staging: • 1: < 25% of the BSA is involved • 2: 25-50% BSA • 3: 50-100%, as erythroderma • 4: vesicles and bullae • Higher stages are more likely to develop chronic skin GVH • Hyperacute GVH: fever, erythroderma (may be pruritic), and desquamation prior to engraftement (before day 14).
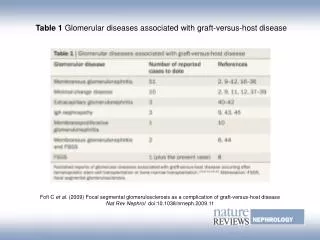
Liver • Next most commonly involved • Cholestatic jaundice; does NOT usually progress to liver failure • DDx: VOD, infection, drug toxicity • The bile duct damage is characteristic, but biopsy is not typically needed. • Staging: • 1: bili 2-3 2: bili 3-6 • 3: bili 6-15 4: bili >15
Gut • Diarrhea (green, water, mucoid; may contain cells and fecal casts), intestinal bleeding, crampy abdominal pain, ileus • Upper tract disease is less common, and occurs in older patients. Requires Bx for diagnosis. • Barium studies show increased transit time and loss of haustral folds • Histology is quite variable. • DDx: residual chemo effects, infection • Staging: • 1: diarrhea 500-1000* cc of stool/day OR persistent nausea • 2: 1000-1500* cc 3: >1500* cc 4: pain +/- ileus *stool volumes were determined in adults.
Grading: the overall deal *officially recorded as “+,” but I find the numbers easier to see
How do we treat GVHD? Prevent it!!
GVHD Prevention • To review briefly: match well (antigens, ?CMV), T-deplete (?), condition less • These suggestions are all very well for GVHD, but have to be balanced with what is good (well, bad) for the underlying disease • Prevent infection • Immunosuppress post-transplant • Consider antibody prophylaxis
Antibody prophylaxis • IVIG helps on 2 fronts • Prevents certain infections • Reduces the frequency of aGVHD, at least in adults • no, I don’t actually know how • ATG has not yet been proven helpful on a sustained basis, but is sometimes used as part of immunosuppression • Other agents such as anti-cytokine products are now being used and tested – more on those if we have time.
Immunosuppress • MTX, the old standby • MTX + CSA • MTX + CSA + PRED • CSA + PRED • CSA • FK506 + CSA • It’s difficult to interpret a lot of this data, as it is either very small numbers or compared across different prep regimens, types of transplant, ages, etc. • Not only the agents, but the doses and length of therapy are all open to question.
Aplastic anemia (non-TBI-based prep) Haploidentical donor – old protocol Haplo, new protocol Unrelated donor, T-depleted graft (with TBI) CSA/MTX CSA/ATG Nothing! CSA/MP taper What do we use? NOTE: Can substitute FK506 (tacrolimus) for CSA in most cases
Prevent infection • An area where the nursing staff has particularly great opportunity to make a difference • BMT diet: NOT proven. SAA patients conditioned with CSA alone benefited from aseptic guts. • Hand washing is well-proven, but not for GVH • Limiting sick staff is a hot topic, again “just” for overall infection • Surveillance cultures are still recommended, and antimicrobials • Mouth cares: may actually be helpful, though it is unclear exactly how infectious mucositis and mucous membrane GVH involvement are related • Matching for CMV: another hot topic, as it may be better from a relapse perspective NOT to.
Initial therapy • Treat all patients with grade II or greater. • Methylprednisolone (IV steroid) is the primary treatment of choice. Boluses may range from 1-60 mg/kg/day. Taper based on response. • Continue GVH prophylaxis (such as CSA) during therapy, plus of course infection prophylaxis (especially TMP/SMX). • CSA is generally not a great treatment, nor ATG. However, some patients will respond, especially to CSA + methylpred.
New kids on the block • Mycophenolate mofetil (MMF, Cellcept) is becoming more established in the treatment of aGVHD. It kills lymphocytes. • Newer on the block is anti-IL-2R, aka anti-CD25, or daclizumab (Zenapax).
Salvage therapies • Anti-TNF-alpha, or infliximab (Remicade), which works for aGVHD (especially gut) but leads to increased fungal infections. (We have mostly used it for cGVHD, here.) • Anti-CD25 (CD25 is a surface marker for activated T cells), or daclizumab (Zenapax): a current NIH study • Many others in adult patients, mostly with around 30% response rates and very poor “cure” rates • Anti-CD3 (anti-T cell) antibodies have been tried in various forms, but thus far with as many complications as successes (for this; they’re useful in solid tumor rejection) • Ultraviolet radiation and psoralens are currently considered “salvage” as well.
Remember when you didn’t want to see this? Don’t you like it better now? graft IL-1 IFN TNF Remicade IL-2 foreign cell (non-self) Zenapax Cellcept
A few words about chronic GVHD • By definition, occurs after day 100, but usually occurs between 3 and 18 mos post-BMT. • 30% of matched-sib transplants (all comers, not just peds) • Around 50% of those with > grade 1 acute GVH will go on to develop chronic GVHD; 10-20% mortality. • In general, diagnosis and treatment are similar to acute; however, grading is usually as “limited” versus “extensive.”
What’s happening now • FK506 (tacrolimus, Prograf) is becoming more important in BMT, and may be particularly successful in steroid-resistant patients. (Probably works by decreasing cytokine production and lymphocyte activation.) • New antibodies and combinations of these newer therapies are keeping the basic science folks busy. Around our campus, cellular therapies are also being studied. • So, in 2-3 years, the amount of information on GVH prevention and/or therapy may double.