Download
1 / 34
340 likes | 354 Views
Learn about the bacterium Clostridium difficile (C. difficile), its risk factors, symptoms, transmission, and prevention measures, including the role of antibiotics and gut immunity.

E N D
PHPU Health Protection Team April2017 Prevention and Control of Clostridium Difficile
Clostridium difficile Clostridium difficile is a bacterium that can be found in people’s intestines (their “digestive tract” or “gut”). However, it does not cause disease by its presence alone; it can be found in healthy people and is widely recognized that infants can be colonized with C. difficile, which can persist during the first 2 years of life (up to 3% of adults and 66% of babies). It causes disease when the normal bacteria in the gut, with which C. difficile competes, are disadvantaged, usually by someone taking antibiotics, allowing the C. difficile to grow to unusually high levels. This allows the toxin they produce to reach levels where it attacks the intestine and causes symptoms of disease.
Etiology and Risk Factors C. difficile spores must be ingested for a person to become colonised and subsequently develop CDI. When the spores enter the colon they germinate into viable bacteria, and, if the strain is toxigenic, produce toxins (toxins A/B) that interact with the epithelium of the gut, which cause damage to the epithelial cells and inflammation of the gut
Etiology and Risk Factors In elderly people, the normal gut flora is less dense and contains fewer bacterial species. This reduces the colonisation resistance to invading pathogens such as C. difficile. Although CDI can be treated with certain antimicrobials, immune function is also very important for the individual patient outcome. Healthy people with no underlying diseases are less likely to develop CDI after ingestion of C. difficile spores. It is recognised that gut immunity declines with increased age
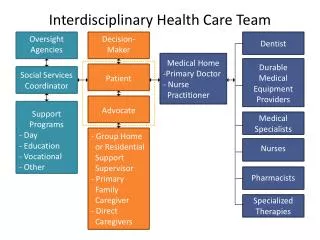
Major risk factors for CDI Certain patients are at increased risk of acquiring CDI. The possibility of CDI should be considered when patients with diarrhoea also have: • Current or recent use of antimicrobial agents • Increased age • Prolonged hospital stay • Serious underlying diseases • Surgical procedures (in particular bowel procedures) • Immunocompromising conditions • Use of proton pump inhibitors
Use of antibiotics and proton pump inhibitors Use of antimicrobial agents (for therapy or prophylaxis) is the main predisposing factor for developing CDI. Prolonged use of proton pump inhibitors may also predispose for CDI. Prudent use of antimicrobial agents is the single most important factor in preventing CDI in the community Prescribers in the community setting should follow local guidance on prescribing antibiotics in the community Proton pump inhibitors should only be used when there is a clear indication
Transmission • As C. difficile is an anaerobic bacterium, viable bacteria will quickly die when exposed to air. However, C. difficile produces hardy spores that can tolerate air, heat and resist various detergents and disinfectants, and are able to survive for extended periods in the environment. • C. difficile is transmitted between people via spores that are picked up either by direct contact with an infected (or contaminated) person or by indirect contact with a contaminated surface. The ability of these spores to survive in the environment, even when disinfectants are used, has contributed to the wide spread of C. difficile in healthcare facilities
Mode of Transmission Chain of Infection
Pathogenesis of CDI C. difficile spores are transmitted by faecal-oral route which, when ingested, find an adequate environment and pH in the bile of the small bowel to germinate into their vegetative forms and subsequently colonize the intestine. Toxin induced damage of the mucosal barrier is the main pathogenic mechanism of C. difficile.
1. Ingestion of spores transmitted from other patients via the hands of healthcare personnel and environment 3. Altered lower intestine flora (due to antimicrobial use) allows proliferation of C. difficile in colon 4. Toxin A & B Production leads to colon damage +/- pseudomembrane 2. Germination into growing (vegetative) form Sunenshine et al. Cleve Clin J Med. 2006;73:187-97.
Symptoms Mild to severe diarrhoea, Blood stained stools, Foul Stool smell Fever and Abdominal cramps
Definition of diarrhoea Diarrhoea is defined as the passage of 3 or more loose or liquid stools per day, or more frequently than is normal for the individual (usually at least 3 times in a 24 hour period). Diarrhoea is usually a symptom of gastrointestinal infection, which can be caused by a variety of bacterial, viral and parasitic organisms. The frequent passing of formed stools is not diarrhoea.
When and how to obtain a faecal specimen from a resident A faecal specimen should be obtained as soon as possible following onset of symptoms of diarrhoea. Preparation for faecal specimen collection: • Gather all relevant equipment • Clean, disposable/reusable bedpan or similar container. • Leak proof sterile specimen container preferably with attached spoon or a clean disposable spatula. • Complete patient details on the specimen container before obtaining the specimen • Leak proof sealable bag (with separate compartment for the specimen). • Laboratory request form (if possible complete patient details before obtaining the specimen).
Procedure 1. Explain the need for the procedure to the resident including the reason for the test (e.g. symptoms of diarrhoea), when and how the results will be given. 2. Ask the resident to pass faeces into the bedpan or container avoiding if possible passing urine at the same time. 3. Put on gloves and aprons to receive the bedpan. 4. Transfer faeces into a leak proof sterile specimen container using the spoon built into the container or a clean spatula to the fill line of the specimen container (or as a minimum covering the cone shape of the container). If the specimen contains blood, pus or mucus try to get these into the container. 5. Put on the container lid and secure. Avoid contaminating the outside of the container. 6. Discard bedpan and contents as usual. Discard other healthcare waste as defined in local policy. 7. Remove gloves and apron and wash and dry hands. 8. Place the specimen container directly into the leak proof sealable bag (The outside of this bag must not be visibly contaminated). 9. Wash and dry hands. 10. Ensure the transport of specimen within 2 hours of collection (If necessary specimens can be refrigerated for up to 24 hours at 4oC in a designated non-food fridge).
Key recommendations The following mnemonic protocol (SIGHT) could be applied when managing suspected potentially infectious diarrhoea: S Suspect that a case may be infective where there is no clear alternative cause for diarrhoea I Isolate the patient and consult with the infection control team (ICT) while determining the cause of the diarrhoea G Gloves and aprons must be used for all contacts with the patient and their environment H Hand washing with soap and water should be carried out before and after each contact with the patient and the patient’s environment T Test the stool for toxin, by sending a specimen immediately
Staff Education • The education should include information on: • Basic pathogenic mechanisms of C. difficile. • Potential reservoirs. • Route of transmission. • Contamination of the environment. • Decontamination of surfaces and equipment. • Hand hygiene. • Use of personal protective equipment.
Isolation precautions Isolation of symptomatic CDI patients is a key step in preventing the transmission of C. difficile • Residents with CDI should be nursed in single rooms (i.e. isolation) with hand washing facilities, en-suite toilet, dedicated care equipment and the door kept closed. • A designated toilet or commode should be provided for each patient with CDI • Personal protective equipment should be put on before entering the isolation room (or area) with symptomatic CDI resident
If isolation in single rooms is not possible, isolation in cohorts should be undertaken • Cohortedpatients should be managed by designated staff, where possible, to minimise the risk of infection to other residents (or staff) • Isolation precautions may be discontinued when the patient has been symptom-free for 72 hrs and bowel movements have returned to normal • Symptomatic CDI residents should not be moved between areas for bed management reasons to minimise the risk of cross contamination
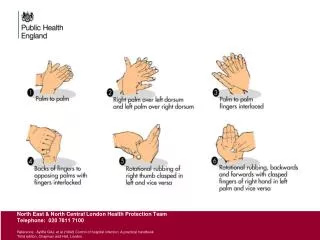
Hand Hygiene Methods Since spores may be difficult to remove from hands even with hand washing, adherence to glove use and Contact Precautions in general should be emphasized for preventing C. difficile transmission via the hands of healthcare personnel Johnson et al. Am J Med 1990;88:137-40.
Hand hygiene • The spread of C. difficile spores via direct and indirect contact is the major route of transmission of CDI in healthcare facilities • Meticulous hand washing with liquid soap and water is recommended for all staff after contact with body substances (including faeces), or following any other potential contamination of hands, e.g., contact with the environment in which a CDI patient is being nursed • Washing of hands using liquid soap and water is recommended after removal of gloves and aprons. Alcohol-based hand rubs are not effective in removing C. difficile spores from hands and should therefore not be the only hand hygiene measure when caring for suspected or confirmed CDI patients • Residents and visitors should be strongly encouraged to wash their hands with liquid soap and water, especially before eating, after using the toilet and when entering and leaving the healthcare facility. The use of liquid soap and water and the physical action of rubbing and rinsing is the only way to remove C. difficile spores from hands
Personal protective equipment • All staff should wear disposable gloves for contact with residents who have diarrhoea including contact with contaminated environment and the immediate vicinity of the resident • The appropriate use of gloves prevents the spread of C. difficile in the care environment and protects members of staff from contamination with spores • Contamination of hands may occur during removal of contaminated gloves therefore hand hygiene remains vital regardless of previous glove use • Disposable plastic aprons should always be used for managing residents who have diarrhoea
Environmental cleaning • Environmental contamination occurs as a result of C. difficile spores being expelled into the environment when patients have diarrhoea. Heavy contamination can be found on floors, toilets, commodes and beds. • When spores have been spread in the environment they may persist for months or years due to their resistance to disinfecting agents, drying and heat.
Environmental cleaning • Regular environmental disinfection of rooms/areas of CDI residents, including frequently touched objects (and surfaces) such as tables, chairs, telephones, door handles etc should be undertaken using a solution with 1000 ppm hypochlorite • Contaminated carpets should be cleaned with detergent and hot water and then either disinfected with hypochlorite (if bleach resistant); otherwise, they should be steam-cleaned • Staff with responsibility for cleaning should be notified immediately when environmental faecal contamination has occurred.
Environmental cleaning • Toilets, commodes and items which are likely to be contaminated with faeces should be cleaned meticulously after use. Particular areas that need to be focused on during cleaning and disinfecting are the seat, back, arms and frame • Soft furnishings that cannot be adequately decontaminated should be discarded. • After discharge of a CDI patient, the resident’s area/room should be cleaned and disinfected thoroughly • Culture of C. difficile from environmental samples is not recommended for routine monitoring of environmental contamination.
Environmental cleaning • An increase in the frequency of environmental cleaning must be undertaken if residents are experiencing diarrhoea. • Products containing a combination of a detergent and hypochlorite are considered the most effective, as hypochlorite alone is not suitable for removing organic matter. • Equipment such as mops and buckets used for cleaning should be colour coded and dedicated to rooms/areas of CDI patients. • For equipment, for example electrical items, that cannot withstand hypochlorite, use other chemical cleaning agents approved by the manufacturer • Corrosion of metal objects (and surfaces) is more likely at higher concentrations of hypochlorite, and vapours can cause respiratory problems. Therefore, the use of concentrations of hypochlorite above 1000 ppm is not recommended.
Safe management of linen • Infected linen –linen that has been used by a resident who is known or suspected to be carrying potentially pathogenic microorganisms. • Soiled/foul linen –refers to linen contaminated with blood or other body fluids, e.g. faeces.
Avoid shaking linen as this may disperse potentially pathogenic • microorganisms and/or skin scales into the environment • Do not wrap items of linen together when disposing of them into a • receptacle. Place each individual item into the bag/receptacle. • All bags should be tied when filled, before transporting. Laundry bags • holding used linen should not be left unsealed/tied • Infected linen bags should never be overfilled and appropriately tagged for • identification • Used linen should not be re-handled or sorted, especially not by carers • in care settings, where laundry facilities are available. • Used linen and linen bags/receptacles should be stored within a designated • area which cannot be accessed by the public and not placed on • inappropriate surfaces. Do not store in corridors
Handling used linen • A disposable plastic apron should always be worn when handling used linen (and disposable gloves where linen is soiled/foul), e.g. during bed-making to ensure contamination from used linen does not occur • Always hold used linen away from yourself to avoid contamination of clothing from linen. • Hand hygiene should be performed following handling of used linen • Ensure appropriate, clean bags/receptacles, e.g. linen buggies, are available as close to the point of use as possible. • Manual soaking/sluicing/handwashing of contaminated items must not be carried out
Soiled items should be placed into soluble alginate bags, then into a colour coded outer bag. • Soiled linen/items such as blankets, sheets, pillowcases should be washed in a separate load using the pre-wash/sluice cycle and at the highest temperature the item can withstand - preferably in a cycle that reaches 65°C for at least 10 minutes or 71°C for at least 3 minutes. • Soiled items which needs to be washed at lower temperatures (e.g. residents’ clothing) should be machine washed with a pre-wash cycle selected, at the highest temperature the item can withstand, along with an appropriate disinfectant added to the washing process (e.g. oxygen releasing or bleaching agent such as sodium hypochlorite added to the penultimate rinse. In the latter’s case, this should be of at least five minutes’ duration, at a concentration of at least 150ppm of chlorine), if tolerated by the fabric.
Storage of clean linen • Clean linen should always be stored in a clean, designated area, preferably a (purpose built) cupboard, away from the floor to prevent contamination with dust and/or aerosols. • Ideally, linen should not be decanted onto different trolleys/shelves or stored in corridors when delivered as this may result in contamination.
Handling of Waste • Waste should be segregated at the point of origin; • Personal protective clothing should be worn when handling waste • Waste should be: • Correctly bagged in the appropriate coloured bag of 225 gauge to prevent spillage • Double bagged where: • The exterior of the bag is contaminated; • The original bag is split, damaged or leaking. • Kept in a rigid-sided holder or container with a foot-operated lid • Only filled to ¾ full • Securely sealed and labelled with coded tags at the point of use to identify their source. • Waste should not: • Be decanted into other bags, regardless of volume • Be contaminating the outside of the bag • Sharps must be disposed of into appropriate colour-coded sharps containers • Sharps container should NEVER be placed into a waste bag.
Health Protection Teams • Provide infection control advice to community facilities as required. • Develop and support the implementation of local policies. • When alerted to an increased number of cases of CDI in adult care homes, the Health Protection Team should initiate further investigations in collaboration with the residential facility/primary care staff