Download
1 / 52
610 likes | 1.2k Views
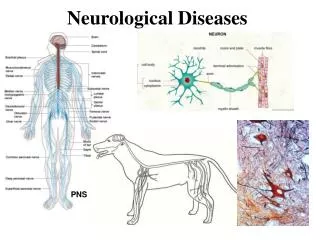
Signs and Symptoms of Neurological Diseases. Berrin Aktekin Department of Neurology. Anatomy - CNS. Cerebral Circulation. Originates from carotid and vertebral arteries. Blood Brain Barrier: Prevents diffusion of toxic substances and large molecules. Neurological Conditions.

E N D
SignsandSymptoms of NeurologicalDiseases Berrin Aktekin Department of Neurology
Cerebral Circulation • Originates from carotid and vertebral arteries. • Blood Brain Barrier: Prevents diffusion of toxic substances and large molecules.
Neurological Conditions • Cardiovascular event – stroke, aneurysm • Encephalitis/ Meningitis • Subdural or Epidural Hematoma • Post-concussion syndrome • Headaches • Seizure/Epilepsy • Cerebral palsy • Neurodegenerative diseases • Dementia • Parkinson • Demyelinating diseases • Multiple Sclerosis – MS • Amyotrophic Lateral Sclerosis - ALS • Peripheral Neuropathy • Guillain-Barre Syndrome • Muscle Disease • Cerebellar Disease
Neurological ExaminationWhat are the components? • Mental Status • Language, Speech • Cognitive assessment • Meningeal irritation • Cranial Nerves • Motor Functions • Reflexes • Deep Tendon reflexes • Superficial cutaneous reflexes • Pathologic reflexes • Sensory Function • Cerebellar Function • Gait
Mental Status • Level of alertness, awareness • Degree of interaction • Orientation • Following commands • Older children: naming objects, simple calculations, extinction, neglect, fund of knowledge • Difference from baseline
Mental Status Assessment • Level of Consciousness (LOC) • alert, • somnolent, • stuporous, • comatose. • Orientation: • person, • place, • time • Memory: • Immediate, • recent • remote
Language, Speech • Language • comprehension • spontaneous, fluent • appropriate content • other things you should check: repetition, naming objects, reading, writing • Speech • prosody • volume • rate • dysarthria
Cognitive Assessment • Thought process • Calculations • Current events • Response to proverbs • Judgment & problem solving ability • Communication abilities • Emotion- Mood and affect
MeninigesCoverings of the Brain & Spinal cord • Meninges: 3 layers tissue • Dura mater • Arachnoid layer • Pia mater • Spaces: • Epidural • Subdural • Subarahnoid
Cerebrospinal fluid: • Contains: • no RBC’s, • few WBC’s, • Glucose 45-75mg/dl, • Protein 15-45 mg/dl.
Cranial Nerves • CN 1: Olfactory…yeah, we don’t check that either • CN 2: Optic • Visual acuity • Visual fields • Fundus • CN 3: Oculomotor • Pupil reactivity to light (direct and consensual) and accomadation • Extraocular eye movements (superior, medial and inferior recti; inferior oblique) • CN 4: Trochlear • Extraocular eye movements (superior oblique) • CN 5: Trigeminal • Muscles of mastication • Facial sensation (V1, 2, 3 divisions) • CN 6: Abducens • Extraocular eye movements (lateral rectus)
Cranial Nerves, continued • CN 7: Facial • Facial muscles • Taste (anterior 2/3) • CN 8: Vestibulocochlear • Hearing • Vestibular function • CN 9: Glossopharyngeal • Taste (posterior 1/3) • Uvula • CN 10: Vagus • Phonation • Palate elevation • CN 11: Spinal accessory • Head turn • Shoulder shrug • CN 12: Hypoglossal • Tongue protrusion
Motor System Voluntary movement • I. motor neuron- upper motor neuron • Extrapyramidal system • Cerebellar system • II. motor neuron- lower motor neuron • Muscular system
Motor System • Strength • Tone • Muscle bulk- Trophy • Reflexes • Deep tendon reflexes • Pathologic reflexes • Superficial cutaneous reflexes • Involuntary movements
Strenght • Check agonist/antagonist pairs • Grading system • 0: no movement • 1: can see muscle contraction but no movement • 2: can move with gravity eliminated • 3: can move against gravity • 4: can resist opposition to some extent, but not full (+, - also) • 5: full strength • Pronator drift: correct position!
Muscle Tone Assessment • Muscle Tone- ranges from flaccid to taut • Atonia - no muscle tone, no resistance • Hypotonia-slight muscle tone, little resistance • Hypertonia- too much resistance • Spasticity- stiff, awkward movements • Rigidity- tightness, inability to bend
Muscle bulk-trophy • Atrophy • Early • II. motor neuron • Late • I. motor neuron • Hypertrophy • Physiologic • Pathologic • Muscular dystrophy
Reflexes • Deep tendon reflexes • Pathologic reflexes • Superficial cutaneous reflexes
Deep Tendon Reflexes Assessment • Deep tendon reflexes- Have pt. in relaxed position, with joint supported. • DTR – compare L to R • Short blow with reflex hammer to the muscle’s insertion tendon (wrist action) • Reinforcement – Have pt. contract muscles not being tested this aids in relaxing muscles to be tested
Scale 0 - 4+ 0 = absent, 1+ = diminished 2+ = average 3+ = brisk 4+ = hyperactive, clonus More pathologic descriptors: crossed, spreading DTR Grading
Pathologic reflexes • Hoffman • Palmomental • Clonus • Sustained • Unsustained • Other • grasp, • suck, • moro, • jaw jerk • Plantar response
Clonus Testing • Perform clonus testing if previous reflex testing reveals Hyperactivity • Relax muscle of calf • Briskly dorsiflex foot and hold stretch • Clonus = rapid rhythmic contractions • NO CLONUS ( no movement) = normal
Superficial Cutaneous Reflex Assessment • Abdominal - Umbilicus shifts toward stimulus. • Cremasteric – Testicle on same side of stimulation rises. • Babisnki (Plantar) – Toes flex.
Involuntary movements: • Tics, • Fasciculations (fine tremors) • Tremors (resting or intentional) • Chorea • Ballismus • Athetosis
Lower vs. UpperMotor Neuron Weakness *Disuse atrophy can develop after initial presentation
Distinguishing Lower Motor Weakness from Muscle Weakness • Weakness due to neuropathy: lower motor neuron disease. • Weakness due to myopathy: nerve function intact.
Sensory System • Five sense !!! • Peripheral Sensory System • Spinothalamic • Dorsal Column • Cortical-integrative Sensory System • Visceral Sensory System
Peripheral Sensory System • Spinothalamicsystem-Cutaneous • Pain- • Temperature • Light touch/pressure • Dorsal Column-Medial Lemniscal System-Proprioception • Vibration • Position
Cortical Sensory Integrative sensation • Graphestesia • Stereognosis • Barognosis • Topognosis • Two point discrimination
Sensory Function Perform all sensory testing with the patient’s eyes closed and test bilaterally. • Components • Light touch • Pinprick • Temperature • Vibration • Joint position sense • Cortical-integrative • Compare sides • Proximal/distal • Right / left • Dermatome • Individual peripheral nerves • Checking a level • Romberg- correct positioning!
Cerebellar Functions • Posture and gait – steady gait with arm swing, balance maintained. • Romberg test – Have pt. stand, feet together, arms side, eyes closed. • Heel to toe gait – tandem walk • Coordination -Corrections of the voluntary motor out-put • Rapid alternating movements • Target finding • Tonus • Hipotonia • Balance • Ataxia
Cerebellar Function Assessment • Rapid Alternating Movements (RAM) Hand movements- Tap finger to thumb, rapidly. Tap each finger to thumb rapidly. Pronate and supinate hands rapidly on knees • Finger to nose test – Eyes closed touch finger to nose alternating and increasing speed • Finger to finger test - Have pt. touch his fingertip to your fingertip, alter position. • Heel to shin test – While supine or sitting, have pt run heel of one foot over the shin of opposite leg • Rebound Phenomen