Download
1 / 31
310 likes | 449 Views
Early Psychosis Optimising Outcomes After the First Episode. PROFESSOR DAVID CASTLE. Chair of Psychiatry, University of Melbourne, St. Vincent’s Hospital Level 2, 46 Nicholson Street, Fitzroy 3065 Tel: (03) 9288 4751 Fax: (03) 9288 4802 Email: david.castle@svhm.org.au.

E N D
Early Psychosis Optimising Outcomes After the First Episode PROFESSOR DAVID CASTLE Chair of Psychiatry, University of Melbourne, St. Vincent’s Hospital Level 2, 46 Nicholson Street, Fitzroy 3065 Tel: (03) 9288 4751 Fax: (03) 9288 4802 Email: david.castle@svhm.org.au
One episode only - No impairment 22% Several episodes with no or minimal impairment 35% Impairment after the first episode with subsequent exacerbation and no return to normality 8% Impairment increasing with each of several episodes and no return to normality 35% The Long Term Course of Psychotic Disorders Figure 2. Graded course of illness in first-admission schizophrenics as indicated by episodes of illness, symptomatology and social impairment at assessments during five years (n=49). Reproduced from Shepherd M, Watt D, Falloon I, Smeeton N. The natural history of schizophrenia: a five-year follow-up study of outcome and prediction in a representative sample of schizophrenics. Psychological Medicine Monograph Supplement 15. Cambridge: Cambridge University Press, 1989.
Broadly diagnosed incident sample of schizophrenia & related disorders Age 15-44yr Relapse After “First Psychosis” (WHO Collaborative Study, 1978-79) (Wiersma et al, 1998) • Gronigen (Netherlands): 15 year ff-up of 85 cases • 2/3 had at least one relapse • 26% “complete remission” • 40% 2 or more episodes with negative syndrome, or chronic psychotic all the time • 11% suicided (Thara et al, 1994) • Madras (India): 10 year ff-up of 90 cases • 53% completely remitted • only 6% continuously psychotic • 4% suicided
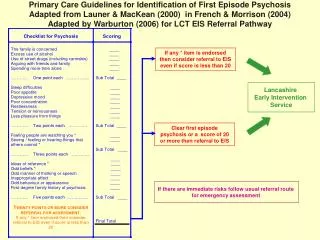
Early Intervention: The Notion of “Untreated Psychosis” “Duration of Untreated Psychosis” (DUP) Table I Treatment lag in five studies of first-episode schizophrenia
Early Intervention: Is it Possible?(A) Problems: - rare disorder - non-specificity of prodromal symptoms Detection Aims
(i) Population-based Educational Interventions • Falloon et al:The Buckingham County Project • intensive intervention over 4yrs • based in English county pop 35,000 with well established health service • mental health teams worked closely with GPs aiming at early referral of all potentially prodromal individuals • use of a screening instrument • referred pts assessed immediately, diagnosis made, education given, then home-based stress management etc. with low-dose neuroleptic for short periods • 4 yr duration of trial: • 1000 referrals • 16 suggestive of prodromal state • 1 schiza • 1 bipolar • Rest: rapid resolution with no long-term sequelae Early Intervention: Is it Possible?(B)
Yung et al (1996):The PACE Clinic, EPPIC, Melbourne concentrated on 16-30yr olds who either: Had a family history of psychosis plus change in mental state indicative of prodrome Developed attenuated psychotic symptoms (eg. Markedly peculiar behaviour; digressive and vague) History of brief transient psychotic episode (<1wk) targeted schools, youth workers referral to Centre for Adolescent Health emphasis on psychosocial and family intervention; tended to avoid neurolepts Early Intervention: Is it Possible?(C) (ii) High Risk Strategy
(ii) High Risk Strategy - Continued • 1st 20 months: 110 referrals: • 56 (50%) from EPPIC • 25 (22%) from community psychiatric clinics • 12 (10%) from schools/tertiary education facilities • 11 (10%) from GPs and health centres • Phone screen: 15 not appropriate • 24 never kept appointment • 71 assessed: 52 (47%) met inclusion criteria • 33 entered research sample • 7 (8%) of total developed frank psychosis Early Intervention: Is it Possible?(D)
May et al: 1st episode admissions to Camarillo State Hospital in 1950’s: patients randomly assigned to either milieu therapy, psychotherapy, ECT, antipsychotics alone or antipsychotics plus psychotherapy. those who received ECT or antipsychotics did best Wyatt (1997): longer-term ff-up of May’s patients: believed those patients ultimately requiring Rx would do worse in long term, but in fact did better (2yr & 6yr) Johnstone et al (1986): Northwick Park study (n=253): longer DUP, worse outcome at 2yrs 120 pts entered placebo/neurolept maintenance trial: DUP better predictor of relapse than medication status Loebel et al (1992): Hillside Hospital series (n=70): longer DUP predicted longer time to remission and lower level of remission (independent of premorbid functioning, age at onset, type of onset) Early Intervention: Is it Worthwhile?(A) (i) Prospective Studies:
Fenton & McGlashan (1987): Chesnut Lodge series: 23pts had good outcome at 15yr ff-up: more likely to have received early treatment. Huber et al (1979): 20 year ff-up of 500 1st psychosis pts entering Bonn Hospital in 1945-1959: 287 received neurolepts or ECT; 213 neither at ff-up, 28% of treatment group were in remission vs. 14% of those not treated those treated within 1yr of onset did best Wyatt (1991): review of 19 studies straddling the introduction of chlorpromazine: early treatment resulted in better outcome, even if no maintenance treatment Haas et al (1994): Study of 150 Schizophrenia pts: worse outcome (positive sx, negative sx, functional impairment) if Rx delayed for more than 2yr Early Intervention: Is it Worthwhile?(B) (ii) Retrospective Studies:
5yr ff-up of 104 people who responded to treatment of 1st episode psychosis Cumulative relapse rates 82% (71%-93%) for first relapse and 78% (47%-100%) for second relapse Halting antipsychotic associated with hazard ratio: 4.89 (2.44 – 9.60) Predictors of poor outcome Poor premorbid functioning in studies and socially Non-predictors of poor outcome sex OCs DUP baseline symptoms neurocognitive function neuroimaging neuroendocrine challenge Outcomes Following “Early Intervention” (A) (Robinson et al, 1999)
180 1st episode patients followed over 3 years 57% remitted but 43% at least one relapse Special intervention benefit for 60%, but 40% “treatment reluctant” and did badly Predictors of poor outcome lack of insight (OR 3.00) non-compliance (OR 2.23) cannabis use (OR 2.28) Outcomes Following “Early Intervention” (B) (Linszen et al, 2004)
What Can Be Done to Optimise Outcomes? (A) Recovery vs. Cure (Barton, 1998) What is a reasonable expectation of “outcome” – “recovery vs. cure” • Symptoms? • Service utilisation? • Quality of life? • Work? • Relationships?
What Can Be Done to Optimise Outcomes? (B) Perpetuating Factors • Suboptimal treatment • psychosis • other symptoms • Poor adherence • Side effects of medication • Substance abuse • High family EE
What Can Be Done to Optimise Outcomes? (C) Individual Issues Needing to be Addressed Positive • Persistent symptoms • Comorbid mood & anxiety disorders • Substance abuse • Medication adherence • Relationships • Healthy lifestyle • Vocational Negative
What Can Be Done to Optimise Outcomes? (D) Treatments That Seem to Work • Optimal pharmacotherapy • Intensive Case Management • Psychoeducation • Family Therapy • Cognitive Behavioural Therapy • “Compliance Therapy” • Social Skills Training • Cognitive Remediation
What Can Be Done to Optimise Outcomes? (E) Collaborative Therapy “A comprehensive therapeutic framework for consumers, clinicians, services and others to work systematically towards the achievement of optimal mental health outcomes”
What Can Be Done to Optimise Outcomes? (F) Collaborative Therapy – Core Module • Initial Assessment / Engagement Process • Group Based Therapy Sessions • 1-1 Therapy Sessions • Collaborative Treatment Journal (CTJ) • Systemic Collaborative Approach • Workshops • Resource Material • Website Support • Data Collection
Structure of assessment packages The MINI Between group ‘catch ups’ Development of one – one component What Can Be Done to Optimise Outcomes? (G) Assessment & Engagement
What Can Be Done to Optimise Outcomes? (H) Group Program Sessions • 10 week intervention, 1½ hours per week • Closed group format • Focus of Self-efficacy • Group Framework • Psycho-education • Coping Strategies • Skills Development
What Can Be Done to Optimise Outcomes? (I) 1-1 Intervention Program • Aim • Provision of an alternative intervention for people unable to participate in groups. Format • Material is adapted from Group Delivery • Sessions by Case Manager • Able to be delivered in 15 minute to 1 hour sessions
What Can Be Done to Optimise Outcomes? (J) Collaborative Treatment Journal (CTJ) • Designed to increase self efficacy of consumer as well as a sense of control over their illness • Increases ability for client to “practice” skills on a 1-1 basis with clinician/case manager thereby adapting skills learned in group to personal environment • Integrated into group based intervention • Relapse prevention tool • Collaborative network
What Can Be Done to Optimise Outcomes? (K) Systematic Collaborative Approach Stress Vulnerability/Self-Efficacy Model Stressors pushing down on Wellness Optimal Level of Wellness Sub-Optimal Level of Wellness Danger Threshold Expression of symptoms impending relapse Coping Strategies
Self-Efficacy & The CTJ (A) My Action Plan – Stage 1 This Action Plan can be used when some of my Early Warning Signs are noticed. My Vulnerable Situations are: (If I have had any of these recently, then watch out for my Early Warning Signs) 1._____________________________________ 2._____________________________________ 3._____________________________________ 4._____________________________________ My Early Warning Signs are: 1._____________________________________ 2._____________________________________ 3._____________________________________ 4._____________________________________
Self-Efficacy & The CTJ (B) My Action Plan – Stage 2 If I notice any of my Vulnerable Situations or Early Warning Signs, and my usual Coping Strategies aren’t effective then I can contact the following people: First contact (eg. your Case Manager, GP etc.): …….....…………………………..…………….....…….. Address:……………………………...………………… Phone:……………………...……………………...…… Second contact: …………………...……..…………….. Address:……………………………...………………… Phone:……………………...……………………...…… Third contact: .……………………………...………….. Address:……………………………...………………… Phone:……………………...……………………...…… If you are unable to make an appointment with any of these people then contact the emergency department of your nearest hospital.
Comprehensive Interventions (Liberman & Kopelwics, 2002) Must appreciate there is no “quick fix” and we require interventions that are “sustained, comprehensive, co-ordinated, collaborative and consumer oriented”.
RCT Elements What Can Be Done to Prevent Relapse? (A) “Episode II” (Gleeson, 2005 on behalf of Episode II Team) • Control • Collaborative Therapy & Family Therapy • realise optimism • psychoeducation • CAT • resilience/strengths • early warning signs • substance use • collaborative with Family & Service Providers • integrate into community care
Phases for Individual Therapy (over 7/12) Family Therapy What Can Be Done to Prevent Relapse? (B) “Episode II” (Gleeson, 2005 on behalf of Episode II Team) • Engagement • Assessment of proximal risk factors (EWS) • Relapse prevention strategies/empowerment • Optional (adherence/substance use/stressful life events/comorbid anxiety or depression) • Coping skills • CBT underpinning approach • includes joint planning session • elements - assessment & history • - Family communication, burden, coping • - Psycho Ed/EWS • - Communication skills/problem solving