Download
1 / 55
590 likes | 808 Views
Endocrine Surgery. Primary Hyperparathyroidism (PHPT). Ca. iPTH. PHPT. PHPT. 0.1-3% of population. Common , over 100 000 new cases diagnosed/y in US. mm. PHPT. Single parathyroid adenoma (80%-90%) Double adenomas (2%-15%) Asymmetric 4-gland hyperplasia (10%-15%)

E N D
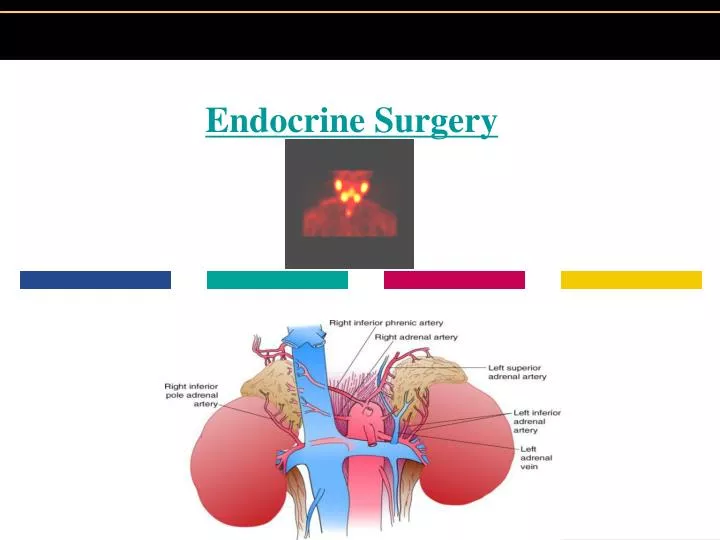
Primary Hyperparathyroidism (PHPT) Ca iPTH PHPT
PHPT 0.1-3% of population. Common , over 100 000 new cases diagnosed/y in US. mm
PHPT Single parathyroid adenoma (80%-90%) Double adenomas (2%-15%) Asymmetric 4-gland hyperplasia (10%-15%) Carcinoma (<1% of patients) mm
Symptoms and Signs • Moans, groans, stones, and bones • Hypercalcemia • Bone disease • Nephrolithiasis • Hypophosphatemia • Proximal renal tubular acidosis • Hypomagnesemia • Hyperuricemia • Gout • Anemia mm
CNS dysfunction Muscle weakness Bowel hypomotility and constipation Peptic ulcer disease Pancreatitis Acute and chronic renal insufficiency Nephrogenic diabetes insipidus Distal renal tubular acidosis Nephrolithiasis Shortening of the QT interval Corneal calcium deposition (band keratopathy) Manifestations of Hypercalcemia mm
Imaging commonly used for cardiac imaging Avidly taken up by parathyroid tissue Reoperative setting A.J. Coakley, A.G. Kettle and C.P. Wells et al., 99mTc sestamibi a new agent for parathyroid imaging, Nucl Med Commun 10 (1989), pp. 791–794 mm
2002 NIH Workshop on Asymptomatic PHPT • Serum Ca > 1.0 mg/dL above the upper limit of normal. • Hypercalciuria (urinary Ca excretion > 400 mg/day) . • Creatinine clearance that is <30% than that of age-matched normal subjects. • Bone density at the hip, lumbar spine, or distal radius that is T score <-2.5. • <50 years old. • Difficult periodic follow-up. mm
IOPTH MEASUREMENTS • Recorded before resection of any enlarged glands • Just before excising the gland. • Postexcision IOPTH levels were measured 10 min or longer after resection of the enlarged parathyroid gland(s). • A decrease of 50% or more in the IOPTH level was used to define successful parathyroidectomy. mm
Why should virtually all patients be considered for surgical intervention? • Surgery offers the only cure • Surgery is of benefit to symptomatic patients • Surgery is of benefit to “asymptomatic” patients • Increases bone density and decreases fracture rates mm
Why should virtually all patients be considered for surgical intervention? • Prolongs survival • Improves neurocognitive symptoms • 92% of patients claim to feel better after parathyroidectomy, even when only 75% claim they felt "bad" before the operation. • Regression of left ventricular hypertrophy. • Cure of diabetes. • Surgical cure rates are high • Surgery is safe mm
Familial HPTH • MEN type 1 • MEN type 2A • Familial Isolated PHPT mm
Surgical approach for MEN1 • Parathyroidectomy • Thymectomy mm
Subtotal parathyroidectomy Total with autotransplantation Subtotal Vs Total with autotransplantation mm
MEN 2A • HPT 20-35% • MTC > 95% • Pheochromocytoma 42-50% • Cutaneous lichen amyloidosis mm
FIHPT • Carefully screened for MEN, including a thorough FHx, ret oncogene testing, and exclude Pit &Panc neuroendocrine tumors. mm
FIHPT • Profound hypercalcemia, Nephrolithiasis, and severe osteoporosis. • No definite genetics have been identified • Jaw tumors (FIH-JT) mm
PHPT in MEN1 • Concurrent ZE syndrome parathyroidectomy (reducing ca levels can reduce gastrin secretion) mm
PHPT in MEN2A • MEN-2A must be biochemically screened for the presence of pheochromocytoma before parathyroidectomy. • If present, parathyroidectomy should be delayed until the pheochromocytoma is addressed. mm
Demographics of Thyroid Cancer • ACS est 20,700 new cases of thyroid cancer in U.S. in 2002 • Cause-specific deaths in 2002 est to be 1300 • Occult cancer in autopsy studies reported to 4-35% worldwide
The New End Point • The gland should be removed en bloc • Care should be taken to remove the entire superior pole • The RLN should be identified and followed to the point where it enters the larynx
Differential Diagnosis of a Thyroid Nodule Nodular hyperplasia Adenoma Cyst Hashimoto thyroiditis Malignancy
Risk Factors for Thyroid Cancer • History of head and neck radiation • Male sex • Family history of medullary carcinoma (MEN syndromes) • Family history of papillary carcinoma • Hoarseness (vocal cord paralysis) • Fixation to adjacent structures • Single, firm, cold nodule • Nodule> 4cm • Rapid tumor growth • Enlarging thyroid nodule(s) on thyroid suppression • Cervical lymphadenopathy
MEN 2 MEN 2A : MTC > 95% of the patients Pheochromocytoma 42-50% Hyperparathyroidism 20-35% Cutaneous lichen amyloidosis MEN 2B: MTC 100% Pheochromocytomas 50% Ganglioneuromas of the lips, tongue, eyelids, and gastrointestinal tract Marfanoid physical (but not cardiac) features mm
Biochemistry Parafollicular C cells CTN CEA Corticotropin Pathology: Amyloid mm
CLINICAL PRESENTATION Most has already metastasized at the time of diagnosis. CLN 15% symptoms of upper aerodigestive tract compression or invasion such as dysphagia or hoarseness 5% distant disease mm
CLINICAL PRESENTATION Calcitonin: Diarrhea facial flushing ACTH: Cushing's syndrome. mm
Genetic screening Patients identified as carriers of a RET mutation will develop MTC and should undergo prophylactic Thyroidectomy. mm
Treatment Total thyroidectomy CLN Dissection: from the level of the hyoid to the innominate vessels and laterally to the carotid arteries. mm
MRND Preserve: SCM Spinal Accessoy N. IJV mm
Pheo & Para in MEN2A MEN-2A must be biochemically screened for the presence of pheochromocytoma before parathyroidectomy. If present, parathyroidectomy should be delayed until the pheochromocytoma is addressed. mm
GeneralCentral obesity*Proximal muscle weakness Hypertension Headaches Psychiatric disordersSkinWide (>1 cm) purple striaeSpontaneous ecchymosesFacial plethora Hyperpigmentation Acne Hirsutism Fungal skin infections S & S mm
Hypokalemic alkalosis Osteopenia Delayed bone age in children Menstrual disorders, decreased libido, impotence Glucose tolerance, diabetes mellitus Kidney stones Polyuria Elevated white blood cell count S & S
5-HIAA • Definitive diagnosis can be confirmed by the finding of elevated urinary 5-HIAA levels • Asymptomatic patients ,only 75% sensitive for detecting the presence of 1ry tumors without metastatic disease. mm
Chromogranin A • Elevated in > 80% of patients with carcinoid tumors. • Elevated level is an independent predictor of an adverse prognosis. mm
CT : hepatic and lymph node metastases SB follow-through: kinking of bowel smooth luminal filling defect Sensitivity:30- 40%. Diagnostic Modalities Capsule Endoscopy mm
Somatostatin receptor scintigraphy: successfully localize primary and metastatic tumors in approximately 80% of patients useful staging procedure before surgical exploration to detect the extent of tumor burden and allow surgical planning. Diagnostic Modalities mm
1ry< 1 cm in diameter without evidence of regional lymph node metastasis: segmental intestinal resection is adequate. Lesions of TI or appendiceal lesios >2cm are best treated by R hemicolectomy. Surgery mm
Gastrinoma • Sporadic 75% • MEN 1 25% • Peptic acid hypersecretion: • abdominal pain • Diarrhea mm mm
12% manifest all three Ps Screen in patient with PHPT who <50y PHPT Pancreatic neuroendocrine tumors: ZES (54%) Insulinoma (21%) Pituitary tumors MEN 1 mm