Download
1 / 17
170 likes | 193 Views
This case study describes a 24-year-old male with acute renal failure and abdominal pain, who underwent renal biopsy. The biopsy findings suggest possible parasitic infection and venous stasis. Additional tests and imaging ruled out renal vein thrombosis and identified potential causes. Follow-up showed improvement in renal function.

E N D
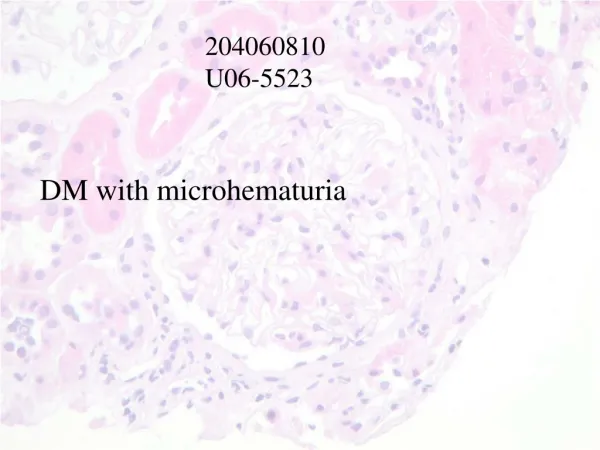
U06-19912 #967529900 • 24 y.o. male • ARF Creat 350 • RBC casts + • Active urine sediment
Renal Biopsy Rounds (November 3): 24 yo Asian male, previously well. ARF Crmax=355(spontaneously resolved) HPI • Sept-Oct: Strenuous training for Edmonton Police Service Exam x several weeks (weight lifting, aerobic exercise) • Unwell x 1 week prior to presentation: URTI and fatigue rests • Few days later: intermittent R sided abdominal pain (no flank pain, no radiation, no hematuria); no N/V/diarrhea • October 18: performs EPS exam to point of exhaustion and syncope x 10 seconds (no preceding SOB/CP/palpitations, no seizure activity) ER. Cr 291 • ROS: No change in urine volume/color, no lower urinary sx. No constitutional/CTD sx. No SOB/orthopnea/edema. No cough/hemoptysis. No NSAIDS/tylenol/steroids/herbs (only whey protein supplements). No IVDU.
No Meds or Allergies. No family hx renal disease. Physical Exam (in ER after 5L NS) 150/90, P82 reg. 99% r/a. Afebrile. 82kg. U/O: 50cc/hr Euvolemic. Normal HS, no edema. Chest clear. Abdo: R mid-quadrant tenderness to moderate palpation; no rebound. No masses. ? Mild R CVA tenderness No rashes or synovitis
Labs [August 31, 2006: sCr=77, urine dip negative] sCr: 291 (Oct 18, 6am) 342 (4:30pm) 355 (Oct 19 6am) despite ++IVf Urine: 3+ Hb, 3+ protein (P/C=268), neg leuks/ketones. 25-50 RBC, 1-2 RBC casts. Una=42, Uosmol=204. FeNa=1.6%. Urine myoglobin cancelled by lab CK 362 265. Troponin -ve Serum lytes N, Ca=2.11, Po4=1.81, Albumin 36. CBC: Hb 149, Plt 255, WBC 12 LFTs, bili, TSH all N. Lipase 371. C3, C4 N. HepB,C,HIV –ve. ANA/dsDNA/ANCA/anti-GBM –ve. EKG: NSR, nil acute. AXR: ++stool; no obstruction/dilatation Renal Ultrasound: N size kidneys, no mass/hydro/stones. October 19: Renal Biopsy
IF • IgG-Negative. • IgA-Negative. • IgM- Mild mesangial staining. • C3- Moderate vascular staining. Mild mesangial staining. • C1q-Negative. • Kappa-Negative. • Lambda-Negative. • Fibrinogen- Moderate interstitial staining. Mild mesangial staining. • Albumin-Negative.
DiagnosisRenal Biopsy: • Patchy severe congestion of glomeruli, arterioles and capillaries with foci of intense polymorph infiltrate. • Rule out parasitic disease.
Comment • Medullary foci of PMN inflammation and intense congestion are quite impressive and unusual • It is likely that there has been considerable regional venous stasis brought about by the disease process (probable parasite forms in the cortex?) that has probably lead to the renal functional impairment
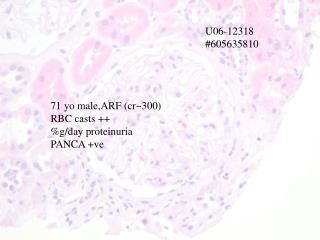
Comment • Renal vein thrombosis seems ruled out by imaging studies. • The congestion suggests that within the kidney there is quite profound venous obstruction or impairment of blood flow.
Schistosoma haematobium • Causes inflammation + fibrosis leading to obstructive uropathy
MRI/MRArenal vessels: normal October 20: sCr 281 October 23: sCr 127 .. October 30: sCr=71