Download
1 / 27
280 likes | 525 Views
Types of injections covered. IM intramuscular IV intravenous (only difficult one that requires more training) intralesional subcutaneous subconjunctival sub- Tenon’s. Most common indications for injections in optometry. IV fluoroescein angiography diabetic retinopathy ARMD

E N D
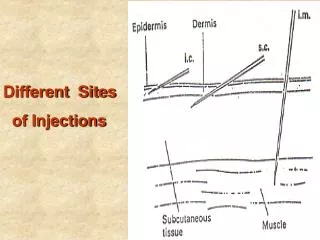
Types of injections covered • IM intramuscular • IV intravenous (only difficult one that requires more training) • intralesional • subcutaneous • subconjunctival • sub-Tenon’s
Most common indications for injections in optometry • IV • fluoroescein angiography • diabetic retinopathy • ARMD • intralesional (most common) • chalazion • Kenalog® (triamcinolone) 40 • 0.1 to 0.3cc injected • subconjunctival • inflammation • IM • to be prepared in the event anaphylactic shock occurs when doing FLAN • epinephrine 1000:1 injected IM
Injectibles billing • FLAN 92235 with ACLS and crash cart • subcutaneous or IM 90782 therapeutic or diagnostic; NOT for cosmesis • intralesional injection for chalazia 11900
Effective infection control • Assume EVERY patient is positive for HIV, HBV, HCV, TB. Take all reasonable precautions to protect yourself, staff from infection. • OSHA requires exposure control plan, etc.
Considerations for bloodborne pathogen controls • (Main) needle stick injuries • sharp container close to location where sharp used • new sharps that reduce possibility of needle stick injuries. • mucous membrane contact • non-intact skin contact • wash hands & wear gloves during injection procedures.
“bottom line for ODs performing injections” • OSHA • Exposure Control Plan • Bloodborne pathogen controls • “get your act together” • review & update annually
Speed of onset for injections (fastest first) • IV • IM (“almost” as quick as IM) • subcutaeous
Considerations when performing fluoroescein angiography • anaphylaxis to IV NaFl • Type I hypersensitivity • IMMEDIATE • May avoid by taking a great history • asthma • allergy • atopic
signs & symptoms to IV NaFl anaphylaxis • *BOARDS* • cutaneous: • hives • itching • angioedema • respiratory • wheezing • tachypnea • cyanosis • tightness in throat • shortness of breath • When above present: • activate EMS • administer EPI pen (1/1000 epinephrine IM) • IM diphenhydraminemay be used for urticaria (hives), itching • monitor vitals ABC’s of CPR supplemental oxygen ifs needed • Trendelenberg position
Anaphylaxis to IV NaFl (Dr. Landgraf’s mnemonic) • SCREAM • S: signs & symptoms of anaphylaxis: • C: cutaneous • urticaria, itch • R: respiratory • wheezing, tachypnea, cyanosis, tightness in throat, shortness of breath • E: EMS activation • call 911 • A: anaphylaxis kit or epi-pen • 1000:1 epinephrine IM; possibly diphenhydramine IM • M: monitor vitals • CPR, supplemental oxygen, Trendelenberg position
General principals about needles for injections • diameter and length • diameter: • size given as “gauge”: • smaller gage larger diameter • larger gage smaller diameter • length: • length varies for purpose: • subcutaneous < intralesional < IM < IV • IM closer to 20 gauge; longer needle • Eye closer to 30 gauge; shorter needle
General principles about syringes • available in different sizes • TB syringe == 1 cc • 3cc, 5cc, 10cc
Main reasons OD would perform IM injection • anaphylaxis to IV NaFl • IM diphenhydramine (Benadryl®) • IM epinephrine (1000:1) • pre or post FLAN for nausea and vomiting • IM phenergan or Compazine • nausea associated with acute angle closure glaucoma • IM phenergan or Compazine • Used for irritating medications • Used for larger volumes (up to 5 ml) or medication
Indications for IV • large volume medications; medical emergencies • FLAN and ICG (indocyanine green) • anaphylaxis IV epinephrine (not used much) • acute angle closure glaucoma IV mannitol • Rule-out Myasthenia Gravis IV Tensilon (ice pack test is just as effective, however)
Specifics about IV NaFl • 100 mg/ml (10%): 5 ml administered (most common) • 250 mg/ml (25%): 2 or 3 ml for eyes with opaque media • 80-90% bound to plasma albumin (only 10-20% free to reach eye)
The dark appearance of fovea in FLAN is caused by … • absence of blood vessels in fovealavascular zone • blockage of choroidal fluorescence due to increased density of xanthophyll at the fovea • blockage of choroidal fluorescence by RPE cells at fovea, which are larger and contain more melanin than elsewhere
Phases of FLAN • ophthalmic artery • short posterior ciliary arteries (fill first) • choroidal circulation • central retinal artery • retinal circulation
IV NaFl: contraindications and warnings • history of previous reaction • asthma • recent stroke, myocardial infarction, unstable angina • pregnancy and lactation • radical mastectomy • renal disease
IV NaFl: Milder? adverse reactions • nausea & vomiting • quick & short lived • extravasation (NaFl leaks out of injection site not in vein; reason why saline is initially injected) • ice packs • dizziness and fainting • pruritis & urticaria (itching & hives)
chalazion management stats • conservative treatment (hot compresses with digital massage) • 40% get better • works well for recent onset chalazion • Intralesional injections alone • 80% • injections + conservative • 90% • incision & curettage • near 100% • ODs do not do this!
chalazion evaluation • how big? • how long? • anterior or posterior to tarsal plate? • injection route conj side (flip lid) OR skin side. • “Rule of sixes” • chalazion > 6 mm; or • duration > 6 months • may not resolve with injection
intralesionalinejctions: complications • Very safe procedure • Very effective procedure • Very easy to do • MINIMAL complications • pain on injection • depigmentation @ site (caution black patients) • bruising • ptosis • vasovagal syncope (faint)
differentiate internal hordeolum vs. chalazion • PAIN • hordeolum is painful • Recurring chalazion?? • sebaceous cell carcinoma
Local anesthetic Xylocaine • subcutaneous injection prior to various procedures • cyst removal or drainage • papilloma and eyelid lesion removal • incision and curettage of chalazion • MOA’s • Xylocaine reversibly blocks nerve conduction temporary paralysis of sensory and motor function with loss of sensation • Epinephrine (1:100,000 not same as EPI pen) vasoconstrictor; prolongs anesthesia decreases systemic absorption & local bleeding
subconjunctival considerations • delivers increased concentration vs. topicals • prolonged tissue exposure • avoid systemic effects • reduce/eliminate compliance issues
subconjunctival indications • refractory uveitis • methylprednisone or kenalog • cystoid macular edema post-op • NSAIDs: Acular, Nevanac, Voltarin, Xibrom • corneal ulcers • trabeculoctomy
subconjunctival contraindications • known hypersensitivity • steroid responders • infectious etiology if using steroids