Download
1 / 9
90 likes | 212 Views
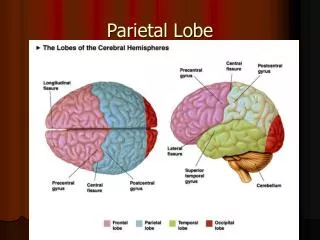
Diagnostic Challenge Pathology for Neurosurgery & Neurology Residents Department of Pathology University of Oklahoma Health Sciences Center, Oklahoma City, OK, U.S.A. Case 6 History: A 60 year-old man presented with an enhancing left parietal mass.

E N D
Diagnostic ChallengePathology for Neurosurgery & Neurology ResidentsDepartment of PathologyUniversity of Oklahoma Health Sciences Center,Oklahoma City, OK, U.S.A. Case 6 History: A 60 year-old man presented with an enhancing left parietal mass. Contributor: Kar-Ming Fung, M.D., Ph.D., karming-fung@ouhsc.edu Last updated: 1/9/2009
Cytologic Preparation Cytologic Preparation A B
Frozen Section Frozen Section C D
Paraffin Section Paraffin Section E F
H I
Glial fibrillary acidic protein (GFAP) p53 J K
Diagnosis: Glioblastoma, WHO IV. • Discussion: • The tumor is composed of highly anaplastic cells with enlarged nuuclei but without prominent nucleoli. The cells have very elongated, fine cytoplasmic processes (arrow in the figure below). Both features are best appreciated with the cytologic preparation. These are features of a glial neoplasm. (Panel A and B) • Necrosis is present (Panel G). This tumor is mitotically active (not shown), has high cellularity, and anaplastic nuclei. (Panel C to I) The overall features are most consistent with a glioblastoma. • Glioblastomas are often but not always immunoreactive for p53. Positive immunoreactivity for GFAP can usually be demonstrated. (Panel I and J) • The bright yellow depositions are hemosiderin that signify prior hemorrhage. The foamy cells are histiocytes which is also a result of prior hemorrhage. (Panel G and H)