Download
1 / 25
250 likes | 448 Views
Audition. December 3, 2008. The Rest of the Way. Production Exercise #4 due at 5 pm today Friday: review + practice spectrogram reading Production Exam: posted as soon as I grade PE #4 due on Friday (5 pm) of finals week Final Exam Reminder: Friday, December 12th 12 - 2 pm

E N D
Audition December 3, 2008
The Rest of the Way • Production Exercise #4 due at 5 pm today • Friday: review + practice spectrogram reading • Production Exam: • posted as soon as I grade PE #4 • due on Friday (5 pm) of finals week • Final Exam Reminder: Friday, December 12th • 12 - 2 pm • SS 541
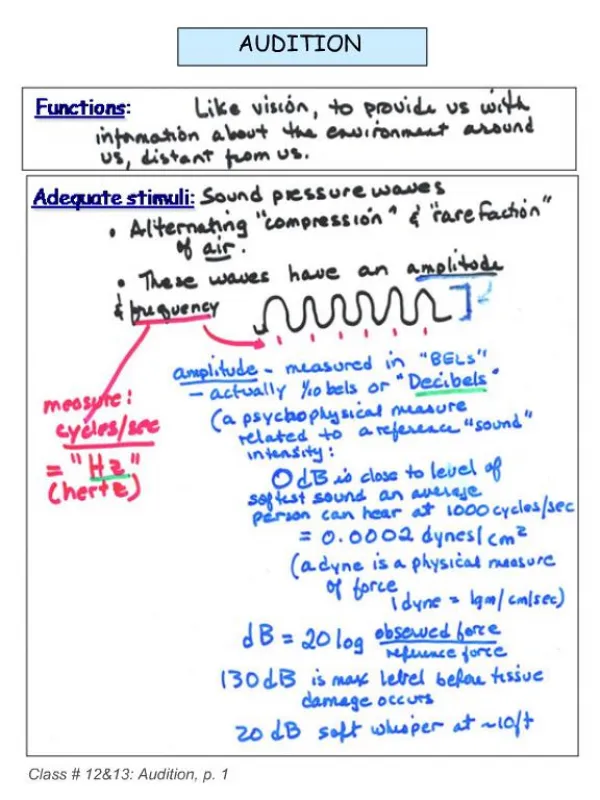
How Do We Hear? • The ear is the organ of hearing. It converts sound waves into electrical signals in the brain. • the process of “audition” • The ear has three parts: • The Outer Ear • sound is represented acoustically (in the air) • The Middle Ear • sound is represented mechanically (in solid bone) • The Inner Ear • sound is represented in a liquid
Outer Ear Fun Facts • The pinna, or auricle, is a bit more receptive to sounds from the front than sounds from the back. • …but basically functions as an “earring holder” • Sound travels down the ear canal, or auditory meatus. • Sounds between 3000-4000 Hz resonate in the ear canal • The tragus protects the opening to the ear canal. • Optionally provides loudness protection. • The outer ear dead ends at the eardrum, or tympanic membrane.
The Middle Ear the anvil (incus) the hammer (malleus) the stirrup (stapes) eardrum
The Middle Ear • The bones of the middle ear act as an amplifier • the “ossicles” • increase sound pressure by about 20-25 dB • Works by focusing sound vibrations into a smaller area • area of eardrum = .85 cm2 • area of footplate of stapes = .03 cm2 • Leverage also factors in… • Like a crowbar.
The Attenuation Reflex • For loud sounds (> 85-90 dB), a reflex kicks in to attenuate the vibrations of the middle ear. • This helps prevent damage to the inner ear… tensor tympani stapedius
The Attenuation Reflex • Requires 50-100 msec of reaction time. • Poorly attenuates sudden loud noises • Muscles fatigue after 15 minutes or so • Also triggered by speaking tensor tympani stapedius
The Inner Ear • The action of the stirrup at the oval window shoves fluid around in the inner ear, including the cochlea • The fluid is electrically charged • Inside the cochlea is the basilar membrane • Different parts of the basilar membrane are maximally displaced by sounds of different frequencies.
How does it work? • On top of the basilar membrane are thousands of tiny hair cells. • Upward motion of the basilar membrane pushes these hairs into the tectorial membrane. • The upward deflection of the hairs opens up channels in the hair cells. • ...allowing the electrically charged fluidof the inner ear to flow in. • This sends a neurochemical signal to the brain.
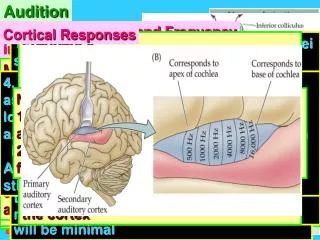
Auditory Frequency Analysis • Individual hair cells in the cochlea respond best to particular frequencies. • General limits: • 20 Hz - 20,000 Hz • Cells at the base respond to high frequencies; • Cells at the apex respond to low. tonotopic organization of the cochlea
Frequency Perception • There are more hair cells that respond to lower frequencies… • so we can distinguish those from each other more easily. • The Mel scale test. • Match this tone: • To the tone that is twice its frequency: • Now try it for a high frequency tone:
The Mel Scale • Perceived pitch is expressed in units called mels. • Note: 1000 Hz = 1000 mels • Twice the number of mels = twice as high of a perceived pitch.
Loudness • The perceived loudness of a sound is measured in units called sones. • The sone scale also exhibits a non-linear relationship with respect to absolute pressure values.
Equal Loudness Curves • Perceived loudness also depends on frequency.
Audiograms • When an audiologist tests your hearing, they determine your hearing threshold at several different frequencies. • They then chart how much your hearing threshold differs from that of a “normal” listener at those frequencies in an audiogram. • Noise-induced hearing loss tends to affect higher frequencies first. • (especially around 4000 Hz)
Deafness • Deafness results when the hair cells of the cochlea die, or do not work properly. • Presbycusis is a natural loss of auditory sensitivity to high frequencies due to age • = loss of hair cells at the base of the cochlea • Note: the “teen buzz” • A hearing aid simply amplifies sounds entering the ear. • (sometimes at particular frequencies) • For those who are profoundly deaf, a device known as a cochlear implant can restore hearing.
Cochlear Implants A Cochlear Implant artificially stimulates the nerves which are connected to the cochlea.
Nuts and Bolts • The cochlear implant chain of events: • Microphone • Speech processor • Electrical stimulation • What the CI user hears is entirely determined by the code in the speech processor • Number of electrodes stimulating the cochlea ranges between 8 to 22. • poorer frequency resolution • Also: cochlear implants cannot stimulate the low frequency regions of the auditory nerve
Nuts and Bolts • The speech processor divides up the frequency scale into 8 (or 22) bands and stimulates each electrode according to the average intensity in each band. This results in what sounds (to us) like a highly degraded version of natural speech.
What CIs Sound Like • Check out some nursery rhymes which have been processed through a CI simulator:
Mitigating Factors • The amount of success with Cochlear Implants is highly variable. • Works best for those who had hearing before they became deaf. • Depends a lot on the person • Possibly because of reorganization of the brain • Works best for (in order): • Environmental Sounds • Speech • Speaking on the telephone (bad) • Music (really bad)
Critical Period? • For congentially deaf users, the Cochlear Implant provides an unusual test of the “forbidden experiment”. • The “critical period” is extremely early-- • They perform best, the earlier they receive the implant (12 months old is the lower limit) • Steady drop-off in performance thereafter • Difficult to achieve natural levels of fluency in speech. • Depends on how much they use the implant. • Partially due to early sensory deprivation. • Also due to degraded auditory signal.
Practical Considerations • It is largely unknown how well anyone will perform with a cochlear implant before they receive it. • Possible predictors: • lipreading ability • rapid cues for place are largely obscured by the noise vocoding process • fMRI scans of brain activity during presentation of auditory stimuli