Download
1 / 21
210 likes | 237 Views
Dive into the anatomy, diseases, classifications, and management of thyroid and parathyroid conditions. Learn about surgical procedures, complications, cancers, and red flag signs. This handbook is a valuable resource for medical professionals at the academic and FY1 level.

E N D
Thyroid, Parathyroid Mo Academic FY1 level 11 Breast and Gynaecology Royal Sussex County Hospital
What you should make use of today • Classification • Eloquence in your presented working diagnosis, differentials and management plan
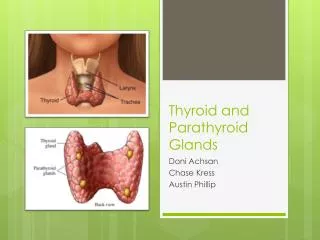
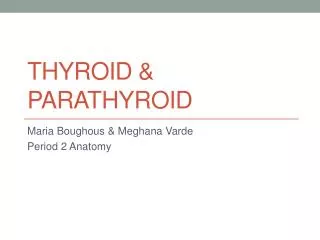
Thyroid • Anatomy • Embryology – Descends from foramen caecum • 3-4th tracheal ring in pre-tracheal fascia • Lobes (pyramidal) and isthmus • 2 pairs arteries (10% ima) 3 pairs veins • Lymphatic drainage – Jug diagastric LN • 4-6 parathyroids
Hx • PC? • Local problems? Lumps? • Hypothyroid sx? • Hyperthyroid sx? • Risk factors – FHx? Radiation? Diet? • Examination
Investigations • Biochemistry – T3/T4/TSH/Ab/ESR • Imaging • FNA/Cytology –Follicular benign/malig? • Tru-cut biopsy • Tc99 • Laryngoscopy
Thyroid disease Congential Acquired
Congenital • Lingual thyroid • Ectopic thyroid – mediastinal op today! • Thyroglossal cyst • Remenants of • thyroglassal duct
Thyroid disease Congential Acquired
Goitres Classify as Diffuse Vs Nodular or Aetiology: Simple • Simple hyperplastic - iodine def ( -->colloid goitre) • Multinodular – UK and euthyroid mx = conservative Toxic • Graves • Toxic multinodular mx = Carbimazole/Propylthiouracil/Radioiodine Propanolol/Thyroxine replacement Inflammatory • Hashimoto’s – Ab and hyper/hypo + lymphoma risk • De-Quervain’s thyroiditis – pain • Reidel’s thyroiditis mx = conservative
Hyper-T3 Surgery? • Subtotal/Total Thyroidectomy • Relapse after > x1 medical mx • Pressure sx • Sx + planning pregnancy Preparing for op: • anti-T3 3months • Stop 10days pre-op • Start iodine
Surgery Complications • Immediate • Primary Haemorrhage • Laryngeal Oedema • Rec Laryngeal + SLN damage • Thyroid storm • Early • Reactionary haemorrhage – tension haematoma • Infection • Hypocalcaemia • Late • Recurrance • Hypothyroid • Stich Granuloma + Keloid
Thyroid Cancer • Benign – Follicular, Cysts, Hyperplastic • Papillary – lymph and multifocal • Follicular – Haem and unifocal and radiosensitive • Medullary – MEN2 parafollicular C • Anaplastic – Very old • Lymphoma – Previous Hashimotos? Non-Hodgkins
Red flag signs in hx? • Family history of thyroid cancer • History of irradiation or exposure to radiation • Child with a thyroid nodule • Unexplained hoarseness or stridor + goitre • Painless thyroid mass enlarging rapidly in weeks • Palpable LN • Insidious or persistent pain for weeks
Thyrotoxic storm Fever >38.5°C, tachycardia, delirium or coma, seizures, vomiting, diarrhoea and jaundice. • It is a clinical diagnosis • Mx: ALS + Sx control + T3 mx
A Anaplastic carcinomaB Follicular carcinomaC Hürthle cell carcinoma D LymphomaE Medullary cell carcinomaF Papillary carcinomaG Spindle cell tumourH Squamous cell carcinoma • 1. A differentiated carcinoma that is derived from the thyroid epithelium, can be associated with the RET proto-oncogene, and is the most common thyroid malignancy. • 2. This malignancy arises from the C cells of the thyroid, and is often associated with MEN2. Carcinoembryonic antigen (CEA) can be used as a tumour marker for this malignancy. • 3. This malignancy is undifferentiated and displays aggressive behaviour with very poor prognosis. • 4. This rare malignancy has a high tendency to metastasise to lung and bone with local lymph node involvement. Histology shows pink-staining enlarged epithelial cells. • 5. Thyroglobulin can be used as a tumour marker for this common thyroid malignancy, which has a tendency to metastasise to the lungs and bone with no local lymph node involvement. It is more common in females than males.
A Anaplastic carcinomaB Follicular carcinomaC Hürthle cell carcinoma D LymphomaE Medullary cell carcinomaF Papillary carcinomaG Spindle cell tumourH Squamous cell carcinoma 1. F 2. E 3. A 4. C 5. B • 1. A differentiated carcinoma that is derived from the thyroid epithelium, can be associated with the RET proto-oncogene, and is the most common thyroid malignancy. • 2. This malignancy arises from the C cells of the thyroid, and is often associated with MEN2. Carcinoembryonic antigen (CEA) can be used as a tumour marker for this malignancy. • 3. This malignancy is undifferentiated and displays aggressive behaviour with very poor prognosis. • 4. This rare malignancy has a high tendency to metastasise to lung and bone with local lymph node involvement. Histology shows pink-staining enlarged epithelial cells. • 5. Thyroglobulin can be used as a tumour marker for this common thyroid malignancy, which has a tendency to metastasise to the lungs and bone with no local lymph node involvement. It is more common in females than males.
Parathyroid • 4-6 glands – inf= 3rdpouch sup= 4thpouch • Hyperparathyroidism • Primary – Solitory adenoma • Secondary – HypoCa ESRF • Tertiary – Autoreg HyperCa ESRF • Sx: Assymptomatic. Bones, Moans and Groans • Ix: Calcium/ALP/Phosphate. Sestamibi + UCCR • Mx: Conservative Vs Surgical
1. A 33-year old woman presents post-partum with a painful red left breast. Fine needle aspiration and cytology shows abundant neutrophils. 2. At Christmas your 53-year old aunt complains of a 2cm by 1cm mobile mass on her right breast that she says has grown recently. You send her to the GP and later discover that on fine needle aspiration it is of a fibroepithelial nature. 3. A 40-year old woman complains of thick green discharge from her right nipple and occasional discharge with blood from the left nipple. On examination there are no palpable breast lumps, but the nipples are retracted. 4. An anxious 42-year old woman presents to her GP as she has noticed bleeding from her right nipple. On examination there is a 0.5cm by 0.5cm mass adjacent to her right nipple and when pressed blood discharges from the same nipple. 5. A 70-year old woman presents with a worsening eczema-like rash overlying the areola and nipples. Upon examination a palpable mass can be felt under the rash.
1. A 33-year old woman presents post-partum with a painful red left breast. Fine needle aspiration and cytology shows abundant neutrophils. 2. At Christmas your 53-year old aunt complains of a 2cm by 1cm mobile mass on her right breast that she says has grown recently. You send her to the GP and later discover that on fine needle aspiration it is of a fibroepithelial nature. 3. A 40-year old woman complains of thick green discharge from her right nipple and occasional discharge with blood from the left nipple. On examination there are no palpable breast lumps, but the nipples are retracted. 4. An anxious 42-year old woman presents to her GP as she has noticed bleeding from her right nipple. On examination there is a 0.5cm by 0.5cm mass adjacent to her right nipple and when pressed blood discharges from the same nipple. 5. A 70-year old woman presents with a worsening eczema-like rash overlying the areola and nipples. Upon examination a palpable mass can be felt under the rash. ANSWERS
Questions? • Clinical skills lab – 27th Oct 5:30-7:30pm • Feedback forms please • A big thank you to Guy and Liam for organising all this