Download
1 / 25

E N D
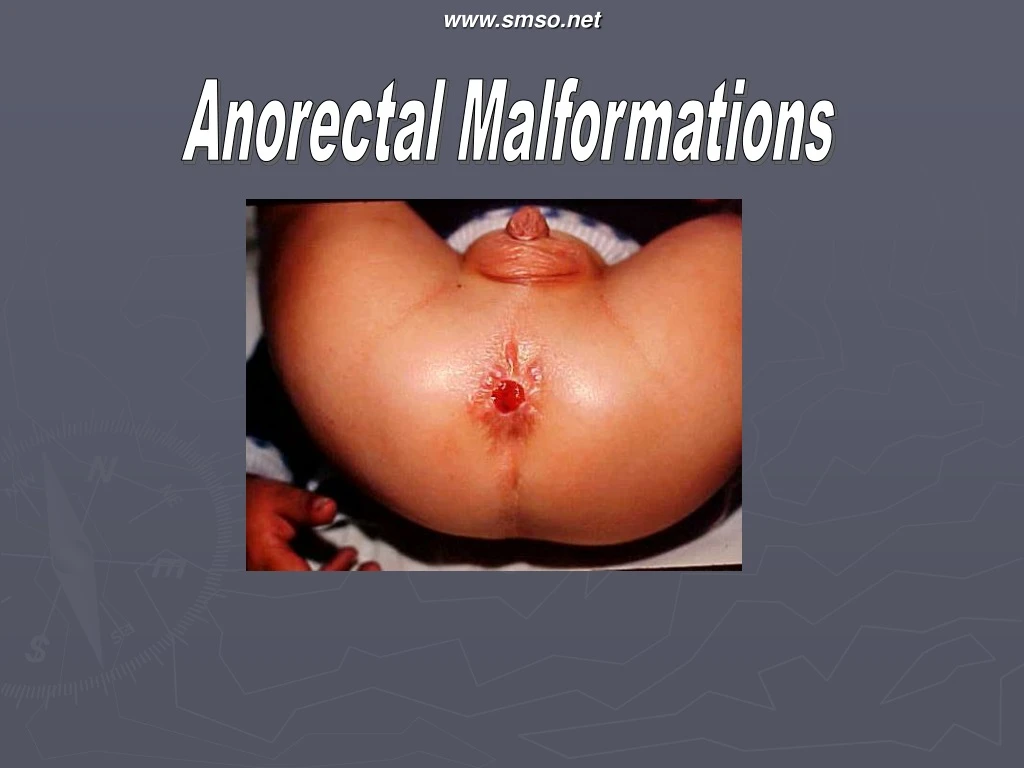
www.smso.net Anorectal Malformations
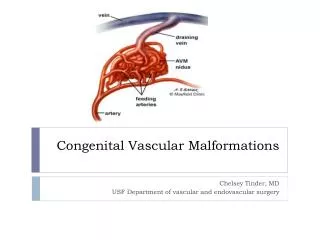
Embryology Early in embryonic life there is a common chamber - the cloaca - into which open the hind gut and the allantois. The cloaca becomes separated into the bladder and post-allantoic gut (rectum) by the down growth of a septum. About this rim an epiblastic bud, the proctodeum, grows in towards the rectum. Normally fusion between these two structures occurs during the third month of intrauterine life www.smso.net
Case Study A 16 year old female patient came with the complaints of passage of stools per vaginum since birth. The patient also gave history of the absence of anal opening since she remembers. The patient had never consulted a specialist for this problem before.The patient had menarche at the age of 12 years and had regular menses. The examination was unremarkable, she had well developed sexual characters.Local examination revealed absence of an anal opening. External genitalia were well developed. Per speculum examination revealed puckering of the left posterolateral wall of the vagina with evidence of faecal matter at the introitus. Per vaginal examination was possible with only one finger .The patient was investigated which were in normal limits. www.smso.net
Anorectal malformation • Absence or an ectopic location of anus • Common congenital anomalies occurring in 1:5000 live births • More often seen in boys than in girls. • 2 types : low & high • Associated anomalies were more common in patients with high type of ARM than in patients with low type of ARM • Long-term prognosis of child with ARM is often more dependent on the extent of these associated anomalies than on the ARM itself www.smso.net
Imperforate anus • covered anus • ectopic anus • stenosed anus • Membranous stenosis www.smso.net
covered anus • The underlying anal canal is covered by a bar of skin with a track running forwards to the perineal raphe. • The track should be opened with scissors, followed by routine dilatation of the anus www.smso.net
ectopic anus • The anus is situated anteriorly and may open in the perineum in boys, or more commonly in the vulva in girls, or rarely into the vagina . • A plastic `cut back’ operation is required (Pena) www.smso.net
stenosed anus • The anus is microscopic, but careful examination usually reveals a minute opening which responds to regular dilatation. membranous stenosis • Here the anus is normally sited, but is covered with a thin membrane which bulges with retained meconium. It is rare, and an incision will cure the condition. www.smso.net
High ARM • Anorectal agnesis • Rectal atresia • Cloaca www.smso.net
Anorectal agenesis • A blind rectal pouch lies just above the pelvic floor — its anterior aspect in the male is attached to the bladder and often there is a rectovesical fistula manifested by the passage of gas or meconium in the urine. In the female, the flstula is usually into the posterior fornix www.smso.net
Rectal Atresia • The anal canal is normal but ends blindly at the level of the pelvic floor. The bowel also ends blindly abovethe pelvic floor without a fistulous opening • This anomaly is rare but must be treated by mobilisation of the rectum and excision of the stricture. After that, end-to-end anastomosis of the anus and rectum must be attempted. More conservative measures are followed by an intractable stricture. www.smso.net
Cloaca • This occurs only in females and here the bowel, urinary and genital tracts all open into a common wide cavity.Commonly severe malformations of the area are associated with other developmental abnormalities, e.g. tracheobronchial fistula. www.smso.net
Management • Thorough physical examination • Decide wither high or low • Radiology • U/A & culture www.smso.net
V: vertebra deformity (most common: sacrum) • A: imperforate anus or anal atresia • C: cardiac anomalies (most common: VSD, ASD, and TOF) • TE: tracheo-esophageal fistula and esophageal • atresia • R: renal or kidney anomalies and radial • anomalies. • L: limb anomalies. www.smso.net
Surgical options • • laparotomy, division of rectourethral fistula and transverse colostomy. A rectal ‘pull-through’ operation can be done later • laparotomy, division of fistula and ‘pull-through’ operation in one stage; division of the fistula and rectal ‘pull-down’ operation through the perineum (this method is now rarely used) • Posterior sagittal rectoplasty (PSARP) (Pena) • colostomy only www.smso.net
Males Anoplasty - Rectoperineal fistula Colostomy - Recto-bulbar urethral fistula, recto-prostatic urethral fistula, rectovesical fistula, imperforate anus without fistula, rectal atresia www.smso.net
Females Anoplasty - Rectoperineal fistula Colostomy - Rectovestibular fistula, imperforate anus without fistula, persistent cloaca, rectal atresia, rectovaginal fistula www.smso.net
THANK YOU www.smso.net