Download
1 / 16
190 likes | 730 Views
Cat Hathaway. cyclic neutropenia Am Report 9/9/2009. Neutropenia. Definition of neutropenia is ANC <1500 cells/mm 3 African american patients can have ANC of 1000 cells/mm3 w/o complications

E N D
Cat Hathaway cyclic neutropeniaAm Report 9/9/2009
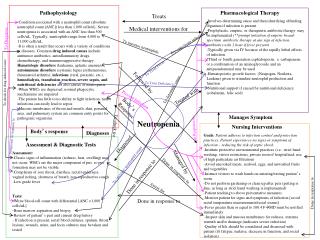
Neutropenia • Definition of neutropenia is ANC <1500 cells/mm3 • African american patients can have ANC of 1000 cells/mm3 w/o complications • Severity of neutropenia determines the risk of infection. Mild is 1000-1500, Moderate 500-1000, and severe <500 • Neutropenia increases risk of bacterial/suppurative infections. Not parasitic or viral infections.
The neutrophil • About 60 billion PMNs are produced DAILY! An equal number are circulating in the blood, the half life is 6-8 hrs. • Neutropenia occurs if bone marrow production lags behind the amount in circulation, from destruction, ineffective granulopoeisis, or shifts into tissue pools/vascular endothelium • Integral in fighting infection of pyogenic bacteria, enteric bacteria, and some fungi
Consequences of Neutropenia • Drug induced granulocytopenia incurs 6-10% mortality rate • Cancer patients with neutropenic fever have 4-30% mortality rate • 21% patients with cancer and neutropenic fever will have serious complications • Patients with ANC <500 will develop severe infxn within 1-4 weeks, ANC <1000 is associated with less risk, but still substantial compared to norms
Congenital neutropenias • Neutropenias associated with immune defects • Congenital neutropenia due to mutations • Cyclic neutropenia • Kostmann Syndrome (Severe Congenital Neutropenia) – Typically die in early childhood • Chronic benign neutropenia • Neutropenia w/ phenotypic abnormalities • Shwachman-diamond-oski syndrome • Cartilage-hair hypoplasia syndrome • Dyskeratosiscongenita • Barth Syndrome • Chediak Higashi syndrome
Congential neutropenia • Benign familial neutropenia • Don’t mount leukocytosis to infection, but are able to mount fever and inflammatory response. Not associated with higher infection incidence • Myeloperoxidase deficiency • Not a real neutropenia, lab error because some labs identify neutrophils based on presence of myeloperoxidase
Cyclic neutropenia • Typically autosomal dominant • Found to be due to germline mutations in ELA2 • ELA2 encodes neutrophilelastase. Interestingly this protein in molecular studies seems to be an oncoprotein • Kostmann syndrome also assoc with ELA2 mutations and GCSF-r mutations and in 10 yrs 21% will go on to develop MDS and or AML • Counts cycle every 21 days with nadirs close to 0 and peaks near normal • Length of nadir relates to infxs complications
Acquired Neutropenia • Infections (most common) • HIV, erhlichia, parasites, parvo B19, EBV, HepB, HCV • Nutritional deficiency • B12, copper, folate • Drugs/chemicals/chemo (1-3.4 cases/million/yr) • Antithyroid, macrolides, procainamide, sulfonamides • Clozapine causes agranulocytosis in 1% of patients, but appears to be genetic not immune • Immunologic due to BMT or blood tx • Felty Syndrome (RA, splenomegaly, neutropenia) • Splenic sequestration • Complement activation (2/2 ECMO, HD, cardiopulmonary bypass, etc)
Other differentials • Leukemia (CLL, CML, ALL, AML, hairy cell) • Lymphoma (Hodgkin, NonHodgkin) • T-LGL – indolent, responds well to immunosuppression • PNH • Bone marrow failure, MDS • MM • Autoimmune Neutropenia (Primary and Secondary) • SLE, RA are assoc with secondary AIN • Primary AIN typically presents in early childhood
Work up • CBC with diff • B12, folate • Infectious workup (if fever present) • Bcx, ucx, cxr, sputum cx • Bone marrow biopsy • Esp if anemia/thrombocytopenia also present • Can evaluate for maturation arrest, fungal infection, marrow defect, b12/folate deficiency • Testing for neutrophil antibodies can be done, but is difficult and false positives and false negatives are common
Neutrophil Antibody Assays • GIFT (granulocyte immunofluorescent test) – indirect assay using patient’s serum and banked normal PMNs • GAT (granulocyte agglutination test) • Normal PMNs incubated with serum from pt • Tests are difficult secondary to HLA alloantibodies and immune complexes • Therefore in routine practice these tests are not recommended
Medications/Treatment • Depends on etiology of neutropenia • Drug related, remove offending agent. • Viral related, no treatment typically necessary • Avoid rectal exams/give stool softener • Neutropenic diet (no fresh fruit/veg) • If fever present then broad spectrum abx • For chemo related or cyclic neutropenia often tx with GCSF agents
Treatment continued • Primary AIN • Typically not associated with severe infections and often only treated symptomatically for infections w/ abx • Secondary AIN • Often assoc with SLE/RA – can use GCSF but have to be careful because this can lead to disease flares and leukocytoclasticvasculitis • Infections due to neutropenia • Management of underlying infxn, supportive abx/treatment
Chemotherapy induced neutropenia • In patients who have developed prior episodes of neutropenia, often will presumptively treat with GCSF as they are at higher risk for recurrent neutropenia • In patients with risk of 20% or more for neutropenia following treatment primary prophylaxis with GCSF may be indicated
Resources • Neutropenia: Differential Diagnoses & Workup. Author: John E Godwin, MD, MS, Professor of Medicine, Chief Division of Hematology/Oncology, Associate Director, Simmons Cooper Cancer Institute, Southern Illinois University School of Medicine Coauthor(s): Christopher D Braden, DO, Attending Physician, Department of Hematology and Oncology, St. Francis Cancer Center, Indianapolis, Indiana. Updated: Oct 16, 2008. Accessed 9/7/09. • Hematology 2004The American Society of Hematology. Congenital and Acquired Neutropenia Nancy Berliner, Marshall Horwitz and Thomas P. Loughran Jr. • Clinical CornerstoneVolume 8, Supplement 5, 2006, Pages S5-S11 Neutropenia: Overview and Current Therapies • Congenital neutropenia Robert L Baehner, MD, Last literature review version 17.2: May 2009 | This topic last updated: March 29, 2009. Accessed 9/9/09 • Overview of neutropeniaRobert L Baehner, MD, Last literature review version 17.2: May 2009 | This topic last updated: February 19, 2009. Accessed 9/9/09