Download
1 / 1
60 likes | 389 Views
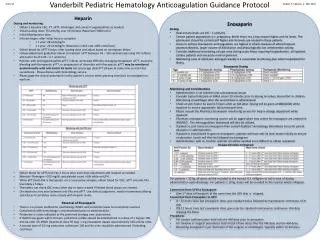
Vanderbilt Pediatric Hematology Anticoagulation Guidance Protocol . 4 / 12/ 12. Robert F. Sidonio, Jr. MD, MSc . . Warfarin Monitoring If inpatient, consider monitoring INRs daily until consistently therapeutic for at least 2 days.

E N D
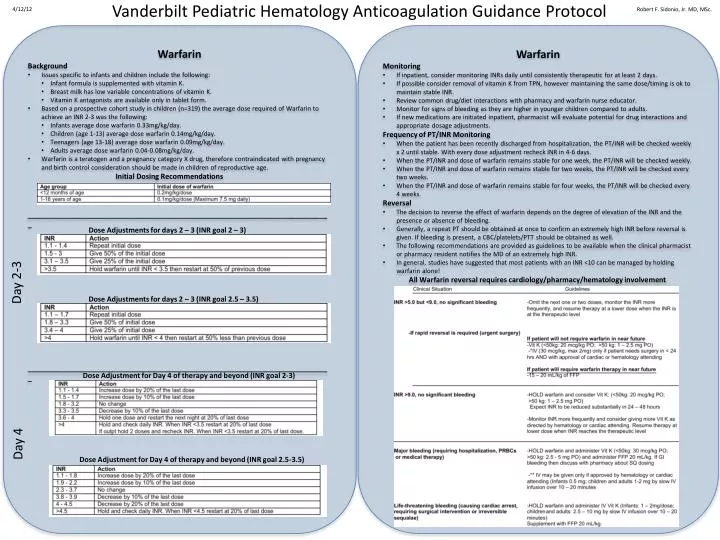
Vanderbilt Pediatric Hematology Anticoagulation Guidance Protocol 4/12/12 Robert F. Sidonio, Jr. MD, MSc. • Warfarin • Monitoring • If inpatient, consider monitoring INRs daily until consistently therapeutic for at least 2 days. • If possible consider removal of vitamin K from TPN, however maintaining the same dose/timing is ok to maintain stable INR. • Review common drug/diet interactions with pharmacy and warfarin nurse educator. • Monitor for signs of bleeding as they are higher in younger children compared to adults. • If new medications are initiated inpatient, pharmacist will evaluate potential for drug interactions and appropriate dosage adjustments. • Frequency of PT/INR Monitoring • When the patient has been recently discharged from hospitalization, the PT/INR will be checked weekly x 2 until stable. With every dose adjustment recheck INR in 4-6 days. • When the PT/INR and dose of warfarin remains stable for one week, the PT/INR will be checked weekly. • When the PT/INR and dose of warfarin remains stable for two weeks, the PT/INR will be checked every two weeks. • When the PT/INR and dose of warfarin remains stable for four weeks, the PT/INR will be checked every 4 weeks. • Reversal • The decision to reverse the effect of warfarin depends on the degree of elevation of the INR and the presence or absence of bleeding. • Generally, a repeat PT should be obtained at once to confirm an extremely high INR before reversal is given. If bleeding is present, a CBC/platelets/PTT should be obtained as well. • The following recommendations are provided as guidelines to be available when the clinical pharmacist or pharmacy resident notifies the MD of an extremely high INR. • In general, studies have suggested that most patients with an INR <10 can be managed by holding warfarin alone! • All Warfarin reversal requires cardiology/pharmacy/hematology involvement • Warfarin • Background • Issues specific to infants and children include the following: • Infant formula is supplemented with vitamin K. • Breast milk has low variable concentrations of vitamin K. • Vitamin K antagonists are available only in tablet form. • Based on a prospective cohort study in children (n=319) the average dose required of Warfarin to achieve an INR 2-3 was the following: • Infants average dose warfarin 0.33mg/kg/day. • Children (age 1-13) average dose warfarin 0.14mg/kg/day. • Teenagers (age 13-18) average dose warfarin 0.09mg/kg/day. • Adults average dose warfarin 0.04-0.08mg/kg/day. • Warfarin is a teratogen and a pregnancy category X drug, therefore contraindicated with pregnancy and birth control consideration should be made in children of reproductive age. • Initial Dosing Recommendations • ____________________________________________________________________________ • ____________________________________________________________________________ Dose Adjustments for days 2 – 3 (INR goal 2 – 3) Day 2-3 Dose Adjustments for days 2 – 3 (INR goal 2.5 – 3.5) Dose Adjustment for Day 4 of therapy and beyond (INR goal 2-3) Day 4 Dose Adjustment for Day 4 of therapy and beyond (INR goal 2.5-3.5)