Download
1 / 128
1.29k likes | 1.62k Views
PSORIASIS. Etymology : Gk, psoriasis , itch. Etiology. Prevalence in is 1-3% and in America and western Lower prevalence rates are found in Japanese and psoriasis is rare in West Africans

E N D
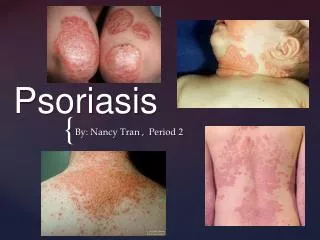
PSORIASIS Etymology: Gk, psoriasis, itch
Etiology • Prevalence in is 1-3% and in America and western • Lower prevalence rates are found in Japanese and psoriasis is rare in West Africans • Psoriasis first appears during 2 peak age ranges:The first peak occurs in persons aged 16-22 years, and the second occurs in persons aged 57-60 years
Pathogenesis • The initiation and maintenance of lesions requires activated T Lymphocytes • Drugs suppressing T-cell activity contribute to the improvement of psoriasis
An unknown antigen may cause Antigen-presenting cells (APCs) to be activated in the epidermis • The APCs internalize and process the antigen, which is then presented on the APC surface • Activated APCs then travel to the lymph nodes and activate naive T cells by binding to it
Binding leads to the recognition of intracellular adhesion molecule-1 (ICAM-1) on the surface of the APC by lymphocyte function-associated antigen-1 (LFA-1) on the surface of the T cell. This interaction sends a necessary but insufficient activation signal to the T cell • Additional costimulatory signals are sent to the T cell as a result of several other interactions • The net effect of all of these signals is an activated T cell with enhanced affinity for endothelial cells
The activated T cell travels along the microvasculature into the dermis and then into the epidermis • In the skin, activated T cells undergo a second activation similar to the previous encounter with APCs in the lymph node • Reactivated T cells then produce cytokines (soluble proteins that can exert both direct and indirect effects on other cells). These cytokines include interleukin-2 (IL-2) and interferon-gamma (IFN-g) • These cytokines induce other cells to produce TNF-a, IL-8, and granulocyte-macrophage colony-stimulating factor (GM-CSF)
Activated T cells and the cytokines cause aborted maturation and excessive proliferation of the keratinocytes. The turnover in the epidermal cells is reduced from 2 weeks to 1 day. These histopathological alterations are clinically evident as plaques
Genetics • Psoriasis was present in 73% of monozygotic twins compared with 20% in dizygotic twins • Psoriasis susceptibility 1 (PSOR1) locus on chromosome 6 is associated with up to 50% of cases • The relative risk of persons bearing the HLA-Cw6 phenotype to develop psoriasis is about 10-fold higher than other persons but only about 10 % of HLA-Cw6 carriers develop psoriasis
When both parents are affected by psoriasis, the rate in siblings is as high as 50%. When one parent is affected, the rate is 16.4% • When neither parent has psoriasis, only 7.8% of siblings of probands are affected • Other studies have shown that 36-71% of patients with psoriasis have one relative who is also affected by psoriasis
Excerbating Factors Can be divided into local and systemic factors. • Local factors 1-Trauma: e g, physical, chemical, electrical, surgical, infective, and inflammatory types of injury or even excessive scratching can aggravate or precipitate localized psoriasis (Koebner reaction)
2-Sunlight: Most patients generally consider sunlight to be beneficial for their psoriasis. Most report a decrease in illness severity during the summer months or periods of increased sun exposure; however, a small minority find that their symptoms are aggravated by strong sunlight
Systemic factors 1-Infection: Pharyngeal streptococcal infections have been shown to produce guttate psoriasis. Some evidence suggests that subclinical streptococcal colonization or overgrowth could be responsible for refractory plaque psoriasis. An increase in psoriasis activity was observed in HIV infected patients. 2-Drugs: Some drugs cause an exacerbation of psoriasis. Lithium and withdrawal from systemic corticosteroids are well known to cause flares of disease. Beta-blockers, antimalarials, and nonsteroidal anti-inflammatory drugs (NSAIDs) have also been implicated.
3-Psychogenic/emotional factors: Many patients report an increase in psoriasis severity with psychological stress. A clear cause-and-effect relationship between disease exacerbation and stress unfortunately has not been proven but, pruritus associated with increased anxiety or depression may promote scratching and a Koebner reaction.
4-Smoking: An increased risk of chronic plaque psoriasis exists in smokers 5-Alcohol: Alcohol is considered a risk factor for psoriasis 6-Endocrine: Psoriasis severity has been noted to fluctuate with hormonal changes. Disease incidence peaks at puberty and during menopause. Pregnant patients' symptoms are more likely to improve than worsenl. In contrast, the disease is more likely to flare in the postpartum period
Clinically Symptoms: • Over 65% of patients complain of itching • Patients may report that their disease worsens in the winter and improves in the summer • The isomorphic phenomenon (Koebner reaction): 38-76% of patients recognize that new lesions appear at sites of injury 7-14 days after the skin has been injured • In some patients, so-called reverse-Koebner reactions have also been noted in which preexisting psoriatic plaques actually clear after injury or trauma to the skin.
Elevated, symmetrical plaques that vary in size from one to several centimeters. They have -Irregular to oval -Sharply demarcated boundaries -Dry, thin, silvery-white scales variable in amount and thickness
-Auspitz sign(Grattage test): Removing the scale reveals a smooth, red, glossy membrane with tiny punctate bleeding points. These points represent bleeding from enlarged dermal capillaries after removal of the overlying epithelium
-Rich red color:often referred to as 'salmon pink‘. This quality of color is of special diagnostic value to differentiate psoriasis from eczema in lesions on the palms, soles and scalp. In the fair-skinned individual, the color is less rich and almost magenta pink. In dark-skinned races, the quality of the color is lost
Clinical patterns1-Psoriasis Vulgaris(Plaque-type) • Seen in approximately 90 % of patients • Single small papules become confluent, forming plaques • Lesions may extend laterally and become circinate because of the confluence of several plaques (psoriasis gyrata)
The borders may resemble a land map (psoriasis geographica) • Annular psoriasis:Ring-like lesions
Elephantine psoriasis is an uncommon form characterized by thickly scaling, large plaques, usually on the lower extremities
Distribution: The extensor aspects of the extremities, particularly the elbows and knees, along with scalp, lower lumbosacral, buttocks, and genitalia. Other sites of predilection include the umbilicus and the intergluteal cleft
2-Guttate Psoriasis(Latin Gutta=drop) • Characterized by eruption of small (0.5 to 1.5 cm in diameter) papules over the upper trunk and proximal extremities • Manifests at an early age • Streptococcal throat infection frequently precedes or is concomitant with the onset or flare
3-Inverse Psoriasis • Localized in the major skin folds, such as the axillae, the inguinal and inframammary areas • Scaling is usually minimal or absent, and the lesions appear glossy • Sweating is impaired in affected areas
4-Psoriatic erythroderma • The disease affects all body sites • Erythema is the most prominent feature with superficial scaling
Patients with erythrodermic psoriasis lose excessive heat because of generalized vasodilatation, and this may cause hypothermia • Psoriatic skin is often hypohidrotic due to occlusion of the sweat ducts • There is an attendant risk of hyperthermia in warm climates • Lower extremity edema is common secondary to vasodilatation and loss of protein from the blood vessels into the tissues
High-output cardiac failure and impaired hepatic and renal function may also occur • Erythrodermic psoriasis may start from worsening of plaque psoriasis to involve most body areas or it may be a response to treatment as a generalized Koebner reaction
5-Pustular Psoriasis • Several clinical variants of pustular psoriasis exist: ِ A-generalized Pustular Psoriasis (Von Zumbusch Type) B-annular Pustular Psoriasis C-impetigo Herpetiformis D-acrodermatitis Continua Of Hallopeau
A-Generalized pustular psoriasis (von Zumbusch type) • It is usually preceded by other forms of the disease • The disease occurs as attacks characterized by fever that lasts several days and a sudden generalized eruption of sterile pustules 2 to 3 mm in diameter
The pustules are disseminated over the trunk and extremities, including the nail beds, palms, and soles • The pustules usually arise on highly erythematous skin, first as patches and then becoming confluent as the disease becomes more severe
The erythema that surrounds the pustules often spreads and becomes confluent, leading to erythroderma • Various provoking factors are known including withdrawal of oral corticosteroids, infections, and irritating topical treatment
B-Annular Pustular Psoriasis • It is a rare variant of pustular psoriasis • Lesions may appear at the onset of pustular psoriasis, with a tendency to spread and form enlarged rings, or they may develop during the course of generalized pustular psoriasis • The characteristic features are pustules on a ring-like erythema
C-Impetigo Herpetiformis • lesions are identical to annular pustular psoriasis but occur during pregnancy • Onset is usually early in the third trimester and persists until delivery • It tends to develop earlier in subsequent pregnancies • It is often associated with hypocalcemia • There is usually no personal or family history of psoriasis
D-Acrodermatitis Continua of Hallopeau • It is rare • sterile, pustular eruption of the fingers or toes slowly extends proximally • Continuous pustulation leads to nail destruction and atrophy of the distal phalanx • It may be associated with generalized pustular psoriasis of the Zumbusch type
6-Sebopsoriasis • It is a common clinical entity • It presents with erythematous plaques with greasy scales localized to seborrheic areas (scalp, glabella, nasolabial folds, perioral and presternal areas, and intertriginous areas)
In the absence of typical findings of psoriasis elsewhere, distinction from seborrheic dermatitis is difficult • It may represent a modification of seborrheic dermatitis by the genetic background of psoriasis
7- Napkin psoriasis • Usually begins between the ages of 3 and 6 months • First appears in the napkin areas as a confluent red area with appearance a few days later of small red papules on the trunk that may also involve the limbs • These papules have the typical white scales of psoriasis
Related Physical Findings 1- NAIL CHANGES IN PSORIASIS • Found in up to 40 percent of patients • Nail pitting is the commonest feature
Onycholysis:white areas of the nail plate due to separation of the nail plate from its underlying attachment to the nail bed • Subungual hyper-keratosis is due to hyperkeratosis of the nail bed
Nail plate crumbling • Beau’s lines:horizontal, lines going across the nail
2-Geographic tongue • Presents as asymptomatic erythematous patches with serpiginous borders, resembling a map • The lesions have a migratory character • It has been postulated to be an oral variant of psoriasis, as these lesions show several histologic features of psoriasis. However, geographic tongue is a relatively common condition and is seen in many nonpsoriatic individuals
3-Psoriatic Arthritis • Develops in approximately 10-15 % of those with psoriasis • In approximately 50% of those affected arthritis appears one decade after the onset of psoriasis, whereas in the remainder the onset occurs with the disease or precedes it
The most distinctive features of psoriatic arthritis are • Distal interphalangeal joint arthritis • Dactylitis
Enthesitis(inflammation of the insertion points of tendons and joints into bone) • Periosteal new bone formation • Asymmetric oligoarthritis& spondylitis • The blue arrow = a normal joint space • Red arrow = “cup and saucer” effect of the fourth metatarsal bone being jammed into the base of the fourth toe • The yellow circle = “Pencil appearance”destruction characteristic of the disease
Modifying Factors • Obesity :Obese individuals are more likely to present with severe psoriasis • Smoking:(<20 cig./day) associated with more than a twofold increased risk of severe psoriasis • Infection: Streptococcal throat infection and guttate psoriasis have been linked • Drugs: Antimalarials, β blockers, lithium, NSAID, imiquimod, angiotensin-converting enzyme inhibitors: Exacerbate psoriasis
Prognosis • Chronic plaque psoriasis is in most cases a lifelong disease, manifesting at unpredictable intervals. Spontaneous remissions, lasting for variable periods of time, may occur in the course of psoriasis in up to 50 % of patients. The duration of remission ranges from 1 year to several decades
Guttate psoriasis is often a self-limited disease, lasting from 12 to 16 weeks without treatment. It has been estimated that one-third to two-thirds of these patients later develop the chronic plaque type • Erythrodermic and generalized pustular psoriasis have a poorer prognosis, with the disease tending to be severe and persistent
PASI Score(Psoriasis Area and Severity Index) • It is a method to estimate severity of psoriasis in order to evaluate the clinical efficacy of new treatments • Psoriatic plaques are graded based on three criteria: redness (R), thickness (T), and scaliness (S) • Severity is rated on a 0-4 scale (0 for no involvement up to 4 for severe involvement) • The highest PASI score is 72; the lowest is 0