Download
1 / 59
600 likes | 683 Views
Autonomic Nervous System: Introduction to neurotransmitter and receptor specificity. Thomas Guenthner Professor of Pharmacology College of Medicine Tel. 996-7635 Room E418, CMW E-mail: tmg@uic.edu. Thanks to Dr. Richard Ye for Powerpoint concepts and slides.

E N D
Autonomic Nervous System: Introduction to neurotransmitter and receptor specificity Thomas Guenthner Professor of Pharmacology College of Medicine Tel. 996-7635 Room E418, CMW E-mail: tmg@uic.edu Thanks to Dr. Richard Ye for Powerpoint conceptsand slides
Knowledge objectives introduced by these two lectures: Identify the key conceptual similarities and differences between autonomic cholinergic and adrenergic pathways including receptor subtypes, neurotransmitters, transmitter synthesis, storage, and release, and relative specificities of drugs that stimulate or inhibit each branch or activity. List the major systems or organs innervated by the autonomic cholinergic and adrenergic systems. Describe the organ system effects of cholinergic and adrenergic stimulation or antagonism. Relate the tissue expression profiles of cholinergic and adrenergic receptors to their specific functions.
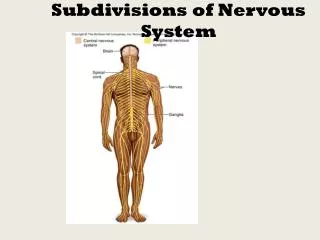
Pharmacological division of cholinergic vs. adrenergic neurotransmission • All preganglionic and parasympathetic postganglionic neurons use acetylcholine as neurotransmitter. Ach is the neurotransmitter at ganglia, nmj, and muscarinic tissue synapses. • Most postganglionic sympathetic neurons use norepinephrine which is an adrenergic neurotransmitter. • There are exceptions: Cholinergic transmission in sympathetic system – all ganglia, adrenal medulla, sweat glads use Ach (nicotinic or muscarinic). Dopaminergic innervation in sympathetic system – renal blood vessels.
Synapse – site most amenable to pharmacologic manipulation: Na+ Precursors (choline/tyrosine) Synaptic cleft Precursor Neurotransmitter Pre-synaptic nerve cell Storage Release Ca2+ Recognition by receptors Metabolic disposition Post-synaptic nerve cell Manipulation possible at pre-synaptic neuron, where neurotransmitter is synthesized, stored and released upon cell activation, or at post-synaptic neuron or effector cell, where neurotransmitter is detected and its action is translated into cellular activities.
Strategies for Pharmacological Intervention: Block synthesis and storage: Usually rate-limiting steps; produce long-term effects Block release: Rapid action and effective Block reuptake increases synaptic neurotransmitter concentrations Can be selective or non-selective Interfere with metabolism: Can be reversible or irreversible; blocking metabolism increases effective neurotransmitter concentrations Interfere with recognition: Receptor antagonists & agonists; high specificity Key Steps in Neurotransmission: Synthesis & Storage Metabolism Action potential Release Recognition (action) Reuptake
Definition of Agonist and Antagonist: Agonist: (1) A natural ligand that activates a receptor. (2) A drug that has properties similar to a natural ligand in activating the same receptor. Antagonist: (1) A receptor-specific blocker. (2) A molecule, such as a drug (e.g., enzyme inhibitor) or a physiologic agent (e.g., hormone), that diminishes or prevents the action of another molecule. Mode of Action: Direct-acting: Molecule that physically binds to the target for its effect. Example: carbachol activates cholinergic receptors. Indirect-acting: Molecule that exerts effect on the target by interacting with another non-target site. Example:neostigmine blocks AchE, causing Ach accumulation. Mode of action and agonism are different concepts. For example, a direct- acting molecule can be either agonistic or antagonistic.
Otto Loewi (Nobel Laureate, 1936) • Discovered that stimulation of the vagus of a frog heart causes release of a substance that, when applied to a second heart, could slow heart rate. He called this “Vagusstoff”, demonstrating the chemical basis of neurotransmission. • Also found that atropine can prevent the inhibitory action, but not the release, of “Vagusstoff”. • Exposure of “Vagusstoff” to frog heart homogenate inactivates it. • Physostigmine enhances the effect of vagus stimulation on the heart, and prevents the destruction of “Vagusstoff”.
CH3 CH3 –CH2–CH2–OH N+ CH3 O CH3 O CoA–S–C–CH3 –C–CH3 CH3 –CH2–CH2–O N+ CH3 Synthesis of acetylcholine: Choline Acetylcholine Choline acetyltransferase + + CoA-SH Acetyl-CoA CoA
ChAT Antiporter Ac-CoA Ach Ach Ach Ach Synthesis, storage and release of acetylcholine: Na+ Choline (10 mM) Synaptic cleft Choline Ach Nerve impulse choline + acetic acid NN Pre-synaptic cell Ca2+ Ach AchE Recognition by receptors Ca2+ NM Post-synaptic cell CAT = choline acetyltransferase AchE = acetylcholinesterase AchE
Steps involved in the action of acetylcholinesterase: 1. Binding of substrate (Ach) 2. Formation of a transient intermediate (involving -OH on Serine 203, etc.) 3. Loss of choline and formation of acetylated enzyme 4. Deacylation of AchE (regeneration of enzyme) Degradation of acetylcholine: H2O O Choline Acetic acid AchE + –C–CH3 (CH3)3 N+–CH2–CH2–OH CH3COOH (CH3)3 N+–CH2–CH2–O (-) OH AchE Glu202 Tyr337 Ser203 Glu334 His447 600,000 Ach molecules / AchE / min = turnover time of 150 microseconds
Ach Drug intervention -- Cholinergic transmission Precursor transport Hemicholinium (Rate-limiting) : Stimulatory : Inhibitory Solid: Agonistic Dotted: Antagonistic Synthesis Cholinergic antagonists Atropine (anti-M) Succinylcholine (anti-NM) Trimethaphan (anti-NN) Storage Vesamicol Release Botulinum toxin Cholinergic agonists (direct acting) AntiChE Carbachol Pilocarpine Reversible (neostigmine) Irreversible (organo- phosphate) Receptor + action Degradation by AchE
An example of indirect agonism: Physostigmine’s effect on acetylcholine receptor is indirect. This effect is mediated through the inhibition of cholinesterase, which causes an increase in the local concentration of acetylcholine. The net effect is agonistic on acetylcholine receptor.
OH Tyrosine hydroxylase CH2 CH2 NH2 NH2 Norepinephrine Dopamine HC HC Phenylethanolamine- N-methyl transferase NH2 NH2 TH Tyrosine DOPA Dopa decarboxylase (L-amino acid decarboxylase) DD (L-AAD) OH CH2 DBH NHCH3 Epinephrine CH CH COOH CH2 COOH CH2 CH2 HO HO HO HO HO HO HO HO HO Dopamine b-hydroxylase Julius Axelrod (Nobel Laureate, 1970) His discoveries concern the mechanisms which regulate the formation of norepinephrine in the nerve cells and the mechanisms which are involved in the inactivation of this important neurotransmitter. Synthesis of Catecholamines 1 3 PNMT Adrenal medulla
Na+ Tyrosine Tyrosine TH DD Dopa Dopamine (DA) DBH NE ATP NE NE Regulation of Norepinephrine Synthesis and Metabolism: a2R Signal Uptake-1 DBH NE ATP NE (-) bR Post-synaptic Ca2+ Pre-synaptic Ca2+ Cellular messengers and effects aR COMT Normetanephrine (NMN) Diffusion, metabolism
NE Drug intervention -- Adrenergic transmission Tyrosine : Stimulatory : Inhibitory Solid: Agonistic Dotted: Antagonistic (Rate-limiting) Metyrosine TH DopaDA Reserpine Adrenergic antagonists Vesicle (DANE) Phentolamine (a-blocker) Propranolol (b-blocker) Amphetamine, tyramine, ephedrine Release Bretylium, guanethidine Adrenergic agonists (direct acting) Cocaine Tricyclic antidepressants (e.g. imipramine) Isoproterenol Albuterol Receptor + action Recapture by Uptake-1
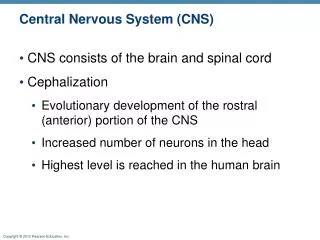
PNS Receptors - Pharmacological Classification: M1, M3, M5 (Gq coupled) Muscarinic R (mAChR) M2, M4(Gi coupled) Cholinergic R NM(neuromuscular, or muscle type) Nicotinic R (nAChR) NN(neuronal, or ganglion type) a2 a1, Adrenergic R b2, b3 b1, D1, D2, D3, D4, D5 Dopamine R Other receptors (receptors for NANC transmitters, e.g. nitric oxide, vasoactive intestinal peptide, neuropeptide Y)
CNS Pre-ganglionic Ganglion Post-ganglionic Effectors Ach Ach Cardiac & smooth muscles, gland cells, nerve terminals Parasympathetic Cranial Muscarinic Nicotinic Ach NE Cardiac & smooth muscles, gland cells, nerve terminals Sympathetic Adrenergic (a, b) Nicotinic Ach Ach Sympathetic Sweat glands Muscarinic Nicotinic Thoracolumbar Ach D Sympathetic Renal vascular smooth muscle Dopaminergic (D1) Nicotinic Ach Sympathetic (adrenal medulla) Released into blood Epi Nicotinic Ach Motor (somatic) Sacral Skeletal muscle Nicotinic Ach = acetylcholine D = dopamine Epi = epinephrine NE = norepinephrine
OH OH CH2 CH2 NHCH3 NH2 Epi NE OH CH CH CH CH2 HO HO HO HO HO HO NH Iso CH(CH3)2 Classification of adrenergic receptors by agonist potency a -- NE Epi > Iso b -- Iso > Epi > NE NE = norepinephrine Epi = epinephrine Iso = isoproterenol
Agonist Agonist Agonist Gi Gs Gq Signaling properties of adrenergic receptors Norepinephrine Methyl NE Clonidine Norepinephrine Epinephrine Phenylephrine Isoproterenol Albuterol (b2) Dobutamine (b1) b1,2,3 a1 a2 cAMP Inositol phosphates (IP3) cAMP Calcium channels Diacyl glycerol (DAG) K+ conductance Mostly excitatory Mostly excitatory Mostly inhibitory
Agonist Agonist bg bg ai ai as as bg bg Gs and Gi proteins have different functions Alpha2 receptor Beta1 receptor AC Gs = stimulatory G protein Gi = inhibitory G protein AC = adenylyl cyclase (convert ATP to cAMP)
Distribution and functions of adrenergic receptors: a1: postsynaptic effector cells, especially smooth muscle Vasoconstriction, hepatic glycogenolysis a2presynaptic adrenergic nerve terminals (autoreceptor), platelets, lipocytes, 0 smooth muscle Inhibition of transmitter release, platelet aggregation, relaxation of gi smooth muscle b1 postsynaptic effector cells: heart, lipocytes, brain, presynaptic adrenergic / cholinergic terminals Increased cardiac rate & force, relaxation of gastrointestinal smooth muscle b2 postsynaptic effector cells: smooth muscle, cardiac muscle Bronchodilation, vasodilation, relaxation of visceral smooth muscle, hepatic glycogenolysis b3 postsynaptic effector cells: lipocytes Lipolysis
Metoprolol Nadolol b2 antagonistic effect half-life Pindolol b1 antagonistic Partial b2 agonistic b1 and b2 antagonistic Propranolol Acebutolol b1 antagonistic Partial b2 agonistic Atenolol b1 antagonistic half-life
OH Tyrosine hydroxylase CH2 CH2 NH2 NH2 Norepinephrine Dopamine HC HC Phenylethanolamine- N-methyl transferase NH2 NH2 TH Tyrosine DOPA Dopa decarboxylase (L-amino acid decarboxylase) DD (L-AAD) OH CH2 DBH NHCH3 Epinephrine CH2 CH CH CH2 COOH COOH CH2 HO HO HO HO HO HO HO HO HO Dopamine b-hydroxylase 1 3 PNMT
Agonist Agonist Gi Gs Dopaminergic receptors in the periphery Dopamine receptors play important roles in CNS. Notably, dopamine neurotransmission is involved in several diseases including Parkinson’s disease, schizophenia, and attention deficiency disorder. There are 5 types of dopamine receptors (D1 – D5). In periphery, D1 dopamine receptor mediates renal vasodilation, and increased myocardial contractility. D1,5 D2,3,4 cAMP cAMP
Cholinergic receptors: Nicotinic Nicotiana tabacum (cultivated tobacco) “Nicotinic actions” -- similar to those induced by nicotine; action mediated by nicotinic cholinergic receptors: • stimulation of all autonomic ganglia (NN) • stimulation of voluntary muscle (NM) • secretion of epinephrine from the adrenal medulla (NN)
Nicotinic acetylcholine receptor: Function Ligand-gated ion (Na+) channel - an “Ionotropic Receptor” • Acetylcholine binds to the a-subunits of the receptor making the membrane more permeable to cations (sodium) and causing a local depolarization. The local depolarization spreads to an action potential, or leads to muscle contraction when summed with the action of other receptors. The ion channel is open during the active state. • Nicotine in small doses stimulates autonomic ganglia and adrenal medulla. When large doses are applied, the stimulatory effect is quickly followed by a blockade of transmission.
Depolarizing Binds and locks the receptor open Nicotinic receptor antagonists Competitive vs. depolarizing Competitive Physically blocks Ach binding INHIBITOR
Cholinergic receptors: Muscarinic “Muscarinic actions” -- reproduced by injection of muscarine, from Amanita muscaria (fly agaric). Similar to those of parasympathetic stimulation Multiple muscarinic cholinergic receptors distributed in different tissues. Therefore, the “muscarinic actions” are dependent on the receptors in different tissues and cells. • Neural/enteric (M1): CNS, ENS, gastric parietal cells (excitatory; Gq) • Cardiac (M2): atria & conducting tissue; presynaptic (inhibitory; Gi) • Glandular/endothelial (M3): exocrine glands, vessels (excitatory; Gq) • Neural (M4): CNS (inhibitory; Gi) • Neural (M5): CNS (excitatory; Gq) • (Sites of primary expression are listed; all are found in CNS)
Muscarinic acetylcholine receptors – G Protein-Coupled Receptors (“Metabotropic” Receptors) Agonist Agonist Gi Gq M1 (enteric, neuronal) M2 (cardiac) M3 (glandular, vascular ) M4 (CNS) M5 (CNS) Mostly excitatory CNS excitation Gastric acid secretion Gastrointestinal motility cAMP IP3, DAG Mostly inhibitory Cardiac inhibition Presynaptic inhibition Neuronal inhibition Ca2+ channel Intracellular Ca2+ (Inhibition) (Stimulation) Glandular secretion Contraction of visceral smooth muscle Vasodilation (via NO) • K+ conductance K+ conductance (Slow IPSP) (Depolarization)
Intracellular signaling triggered by acetylcholine in the Heart Main molecular players: M2, heterotrimeric G Protein Gi, Adenylyl cyclase
Clinical manifestation of excessive cholinergic effects (DUMBELS) D – Defecation U – Urination M – Miosis B – Bradycardia E – Emesis L – Lacrimation S – Salivation
Effects of muscarinic antagonists • “DRY AS A BONE, RED AS A BEET, MAD AS A HATTER.” • Decreased sweating, salivation and lacrimation • Reflex peripheral (cutaneous) vasodilation to dissipate heat (hyperthermia) • CNS effects of muscarinic inhibition -- restlessness, delerium, hallucination • ALSO: • Bronchodilation • Tachycardia • Mydriasis (pupil dilation) and Cycloplegia (loss of focus) • GI and Bladder atony
Physiological Effects of ANS Stimulation and Inhibition
Receptor distribution and effects in the autonomic nervous system: Sympathetic Organ Receptor Parasympathetic Receptor Heart SA node Atrial muscle AV node Ventricular muscle M2 M2 M2 Rate Force Automaticity Automaticity Force 1 b1 b1 b1 b1 Rate Force Conduction velocity AV block Blood vessels Arterioles Coronary Skeletal muscle Viscera Skin Brain Erectile tissue Salivary gland Contraction Relaxation Contraction Contraction Contraction Contraction Contraction Contraction Relaxation a1 b2 a1 a1 a1 a1 a1 a1 b2 M3 M3 M3 Relaxation Relaxation Vein (Continued, next page)
Organ Sympathetic Receptor Parasympathetic Receptor Viscera Bronchiolar SMC Glands GI track Smooth muscle Sphincters Glands Uterus Relaxation Motility Contraction Contraction Relaxation b2 Contraction M3 Secretion Motility Relaxation Secretion Gastric acid secretion Variable M3 M3 M3 M3 M1 a2, b2 a1 a1 b2 Skin Pilomotor SMC a1 Contraction (piloerection) a1, b1 Salivary glands Secretion Secretion M3 Lacrimal glands Secretion M3 b1 Kidney Renin release b2, a1 2, a1 Glycogenolysis Gluconeogenesis Liver b3 Lipolysis Fat From: Rang et al. Pharmacology, 6th Ed. p. 169. Also, see Katzung, Basic & Clinical Pharmacology, 10th Ed. p.86.
Cardiovascular Pharmacology (Blood Pressure)
Cardiovascular effects of intravenous infusion of epinephrine, norepinephrine, and isoproterenol in man. Norepinephrine (predominantly a-agonist) causes vasoconstriction and increased systolic and diastolic BP, with a reflex bradycardia. Isoproterenol (b-agonist) is a vasodilator, but strongly increases cardiac force and rate. Mean arterial pressure falls. Epinephrine combines both actions.
Sir Henry Hallett Dale (Nobel laureate, 1936) (Arterial pressure of an anesthetized cat was measured) Two kinds of effects produced by Ach. A. Ach causes a fall in BP due to vasodilation. B. A larger dose of Ach also produces bradycardia, further reducing BP. C. Atropine blocks the effect of Ach in lowering BP. D. Still under the influence of atropine, a much larger dose of Ach causes a rise in BP and tachycardia. A, B: Muscarinic effects of Ach (M3, M2) C: Muscarinic antagonistic effect (M) D. Stimulation of sympathetic ganglia (NN)