Download
1 / 67
730 likes | 1.35k Views
Genitourinary Trauma. Queen’s University. QUEST 2004. GU Trauma Objectives. ~ 10% of E.R. trauma visits Often associated with multi-system trauma Subtle presentations, easily overlooked Diseased GU organs susceptible to injury. GU Trauma General Considerations.

E N D
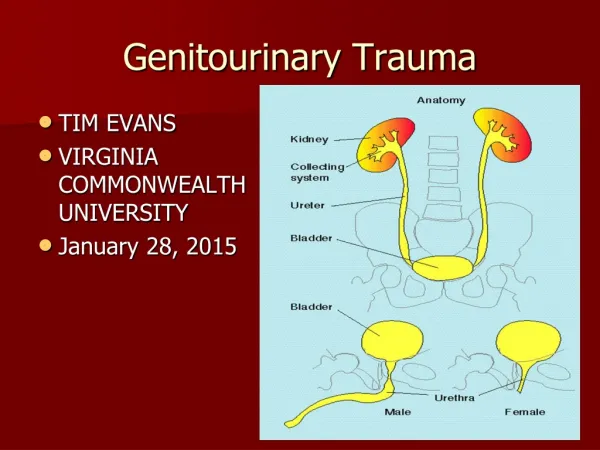
Genitourinary Trauma Queen’s University QUEST 2004
GU Trauma Objectives • ~10% of E.R. trauma visits • Often associated with multi-system trauma • Subtle presentations, easily overlooked • Diseased GU organs susceptible to injury
GU Trauma General Considerations • ~10% of E.R. trauma visits • Often associated with multi-system trauma • Subtle presentations, easily overlooked • Diseased GU organs susceptible to injury
GU Trauma Evaluation • Airway • with C-spine protection • Breathing • Circulation • control of external hemorrhage, 2 large bore IVs • Disability • assessment of neurologic status • Exposure / Environment • undress / temperature control
Case #1 • 36 y/o male multiple stab wounds • Abdomen and L flank • Brought into E.R. by ambulance • C/o L flank and abdominal pain • Question: What would you do next?
Case #1 Hint: Remember those 3 letters…
Case #1 • DPL • DRE • PSA • ABC’s The answer is obvious, but don’t forget it!
Case #1 • ABC’s • P 100, BP 100/60, RR 20 • Vitals maintained with IV resuscitation • Hb = 99 g/L • C/O ongoing LUQ and L flank pain • Signs of peritonitis on P/E • Gross hematuria • Question: What would you do next?
Case #1 • DPL • Transfuse 2 units pRBC’s • CT scan • Laparotomy
CT + IV contrast Delayed images
Case #1 • O.R. • Trauma laparotomy • Ongoing attention to ABC’s • Findings: • Small bowel perforation (no gross spillage) • L retroperitoneal hematoma • All other organs normal, specifically no other source of bleeding • General surgeon repairs SB perforation, then calls for intra-op urology consult • Question: What would you do?
Case #1 • Assess retroperitoneal hematoma • ? Expanding…NO • ? Pulsatile…NO • Need to consider patient status • Hemodynamically stable • What would you do?
Case #1 • Explore retroperitoneum for removal of kidney • Explore retroperitoneum for repair of kidney • Explore retroperitoneum and improvise • Do NOT explore retroperitoneum, but place ureteral stent • Do NOT explore retroperitoneum, no stent
Case #1 • Options: • “Aggressive” approach • Explore retroperitoneum/kidney • Debridement / hemostasis / collecting system repair • “Conservative” approach • With or without ureteral stenting
Renal Trauma General Considerations • Most commonly injured GU organ • Often in association with multi-system organ injury • Blunt >80% • Penetrating <20%
Renal Trauma Blunt • Most common form of renal trauma • Types of injury • Motor vehicle accidents • Falls from heights • Assaults • Mechanisms of injury • High velocity impact (contusion / hematoma / laceration) • Deceleration injury (RA thrombosis / RV disruption / avulsion of renal pedicle)
Renal Trauma Penetrating • Uncommon form of renal trauma • Types of injury • Gunshot wounds • Stab wounds • Mechanisms of injury • Direct shearing force through renal tissue
Renal Trauma Presentation • Hematuria (gross or microscopic) • Microscopic = 5 RBCs/HPF • May be absent • Shock (hypotension, tachycardia, oliguria) • Flank bruising/mass • Flank pain/tenderness
Renal Trauma Indications for Imaging • Penetrating injuries • Blunt injuries in association with: • Gross hematuria • Microscopic hematuria and shock (SBP < 90) • Microscopic hematuria in children • Microscopic hematuria in patient with solitary kidney • Absence of hematuria but high clinical index of suspicion of renal injury based on Hx, Px and AXR • Rapid deceleration injury • Lower rib # • Transverse process # • Loss of psoas shadow
Renal Trauma Options for Imaging Consider the need for both anatomic and functional information • IVP - “Single-shot” intra-op • U/S - Confirm 2 kidneys • Angiography - Used for embolization These modalities have a limited role and have been essentially replaced by CT scan
Renal Trauma CT Scan • Provides valuable anatomic and functional information • Provides the most definitive staging information • Provides information on associated injuries • Imaging modality of choice for renal trauma
Renal Trauma CT Findings – Major Trauma • Urinary extravasation medial to kidney • Suggests UPJ avulsion or renal pelvic injury • Hematoma medial to kidney, displacing it laterally • Suggests pedicle injury • Lack of contrast enhancement of kidney • Suggests arterial injury
Renal Trauma Classification • Many classification systems available • Recommend: • American Association for the Surgery of Trauma (AAST) Organ Injury Severity Scale • Because: • Most widely used • In Campbell’s
Renal Trauma Classification AAST
Pediatric Renal TraumaConsiderations • Occupies proportionately larger space • Less perirenal and subcutaneous fat • Renal capsule, Gerota’s fascia and perirenal fat less developed (? less fixation) • Vascular pedicle more susceptible to shearing forces • Higher catecholamine output after trauma
Pediatric Renal Trauma Controversies • What is appropriate investigation of suspected renal injuries? • What is the significance of degree of hematuria? • Does the rule of microscopic hematuria and shock still fit?
Pediatric Renal TraumaSummary • Shock not a useful parameter • Hematuria may not be present ~10% • Not all children with blunt trauma need to be evaluated but... • High index of suspicion based on mechanism • “Liberal” use of imaging studies
Renal Trauma Non-operative Management • Conservative management for: • 90-98% of blunt renal trauma • Up to 50% of penetrating renal trauma • ABCs • Admission • Bedrest until gross hematuria clears • Close clinical observation • Serial vital signs, CBC
Renal Trauma Indications for Surgical Exploration • RELATIVE • Penetrating injuries • Extensive urine extravasation • Grade 5 injury • “Shattered kidney” • Pedicle injury • Non-viable tissue (>20%) • Arterial injury (main or segmental) ABSOLUTE • Persistent renal bleeding with hemodynamic instability • Expanding perirenal hematoma • Pulsatile perirenal hematoma
Renal Trauma Principles of Surgical Exploration • Transabdominal midline laparotomy • Early control of renal vessels • Exposure of kidney • Open Gerota’s fascia • Dissect kidney from surrounding hematoma • Decision: repair of kidney vs. removal of kidney
Renal Trauma Principles of Renal Reconstruction • Complete renal exposure • Debridement of non-viable tissue • Hemostasis • Suture ligature • Gelfoam, Surgicel • Argon beam coagulation • Water-tight closure of collecting system • Approximation/coverage of parenchymal defect
Renal Trauma Technique of Renal Reconstruction
Renal Trauma Complications • Early • Hemorrhage, shock • Urinoma • Late • Infection • Loss of renal function • Hypertension • BP checks with family doctor
Case #2 • 60 y/o male presents to the E.R. • Intoxicated, c/o diffuse abdominal pain • Tripped down stairs leaving the bar 1 hour ago • Feels the urge to void but is unable • What would you do now?
Case #2 • ABCs • VSS, C-spine exam normal • Guarding and rebound tenderness in all quadrants • DRE normal • Foley catheter inserted • Gross hematuria • What would you do next?
Case #2 • CT Scan abdomen and pelvis • Free fluid • LKKS normal • What additional investigation(s) would you order?
Bladder Trauma General Considerations • Relatively uncommon • Often in association with multi-system organ injury • Significant mortality rate (10-20%) • Have high index of suspicion of urethral disruption injury • Bladder more susceptible to injury when full
Bladder Trauma Etiology • Blunt • Penetrating • Iatrogenic • Spontaneous rupture
Bladder Trauma Etiology BLUNT • Most common type of bladder injury • Usually motor vehicle accidents • 2/3 contusions, 1/3 ruptures • Associated with pelvic # • 10-25% of pelvic #’s have associated bladder injury • 85-90% of bladder injuries have associated pelvic # PENETRATING • Less common • Often associated with major organ injuries
Bladder Trauma Etiology IATROGENIC • Open or laparoscopic pelvic surgery • Gynecologic, vascular, urologic or general surgery SPONTANEOUS RUPTURE • Underlying pathology • Cancer, obstruction, XRT, TB, sensory neurologic deficit
Bladder Trauma Presentation • Hematuria • 95% blunt injuries have gross hematuria • Inability to void • Abdominal pain • Abdominal bruising • Pelvic mass • Peritoneal signs • Shock
Bladder Trauma Imaging • Cystogram • AP films ± obliques • Remember drainage films • 10% of bladder ruptures detected on drainage films • CT Cystogram • Often more efficient since most patients need CT anyway • Provides additional helpful information about other organs
Bladder Trauma AAST Organ Injury Severity Scale • Grade 1: Hematoma (contusion, intramural hematoma) Laceration (partial thickness) • Grade 2: Laceration (extraperitoneal, <2cm) • Grade 3: Laceration (extraperitoneal, 2cm) Laceration (intraperitoneal, <2cm) • Grade 4: Laceration (intraperitoneal, 2cm) • Grade 5: Laceration (intra- or extraperitoneal, extending into bladder neck, ureteral orifice, trigone) Advance one grade for multiple injuries up to grade 3
Bladder Trauma Practical Classification • Contusion • Most common • Often diagnosis of exclusion • Laceration/rupture • Extraperitoneal vs. This is what we really need to know • Intraperitoneal
Bladder Trauma Management GENERAL PRINCIPLES • ABCs • Establish urinary drainage/diversion • Antibiotics CONTUSION • No specific therapy required
Bladder Trauma Management EXTRAPERITONEAL RUPTURE • Conservative, catheter drainage x 7-14 days, cystogram • Indications for surgical repair: • Patient already in O.R. for another reason • Associated rectal perforation or open pelvic fracture • Bone fragments projecting into bladder • Multiple/large ruptures
Bladder Trauma Management INTRAPERITONEAL RUPTURE • Surgical repair • Midline laparotomy/cystotomy • Multi-layer closure of bladder injury • Bladder drainage • Foley catheter ± suprapubic catheter • Perivesical drain
Bladder Trauma Complications • Intraperitoneal • Urinary frequency • Shock • Peritonitis • Azotemia • Extraperitoneal • Shock • Pelvic abscess
Case #3 • 46 y/o woman undergoes TAH-BSO for severe endometriosis • Significant bleeding intra-op, requires 4 units pRBCs • POD# 4: • Still not able to tolerate solids • C/o R flank pain • T=38.6°C • What would you do now?