Download
1 / 31

E N D
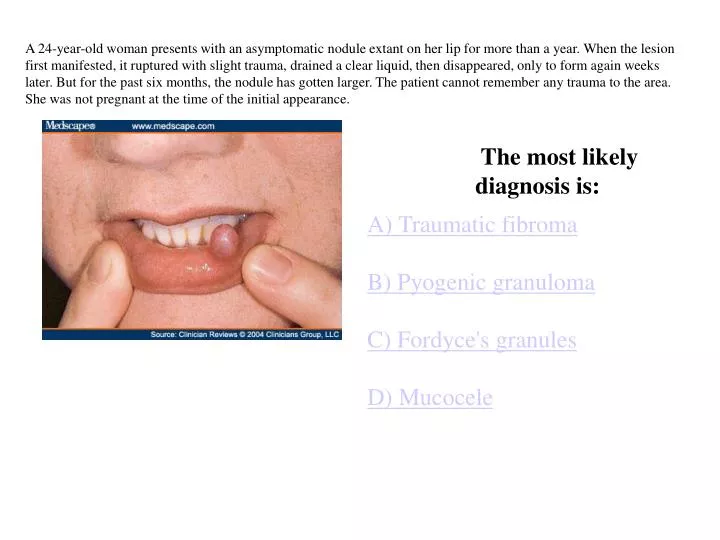
A 24-year-old woman presents with an asymptomatic nodule extant on her lip for more than a year. When the lesion first manifested, it ruptured with slight trauma, drained a clear liquid, then disappeared, only to form again weeks later. But for the past six months, the nodule has gotten larger. The patient cannot remember any trauma to the area. She was not pregnant at the time of the initial appearance. • The most likely diagnosis is: • A) Traumatic fibromaB) Pyogenic granulomaC) Fordyce's granulesD) Mucocele
A 55-year-old man presents with darkening of his facial skin, which he reports has been worsening during the past two years. He did not notice the discoloration until friends pointed it out, and he is otherwise asymptomatic. History reveals that the patient has been taking minocycline for several years for treatment of rosacea. Otherwise, he is in good health; findings from a recent physical examination and related blood tests were all normal. Nonetheless, he requested and received a referral to dermatology. Examination of the skin shows definite bilateral, patchy, slate-colored macular areas of hyperpigmentation, particularly on the sides of the face. There is no epidermal disturbance (ie, scale, broken skin, papularity) in these areas. Examination of his ears, teeth, gums, and sclerae reveal no abnormality. • A) OchronosisB) HemochromatosisC) Drug reaction to minocyclineD) Addison's disease
A 27-year-old woman is referred to dermatology for evaluation of a recurrent "staph infection of the eye," always manifesting in the same location (just below the right eye), always tingling and itching, with slight pain, and always resolving in 10 to 14 days. She has experienced premonitory symptoms with each episode, at which point she has sought medical evaluation and been given oral antibiotics. While the treatment seems effective, the problem persists. She is an otherwise healthy individual and is not prone to skin infections in general, although she has had cold sores. Examination reveals a collection of papulovesicular lesions on an erythematous base below the right eye. There is no adenopathy in the area, and the eye itself is not involved, nor has it been during past episodes • A) Recurrent staph infectionB) Recurrent shingles (varicella-zoster virus)C) Contact dermatitisD) Herpes simplex virus
70-year-old man is referred to dermatology for evaluation of "ringworm" on his legs and trunk, which has been unresponsive to topical and oral antifungal medications. The lesions initially manifested in the early fall and increased in number with the onset of winter. The patient owns no pets or livestock and has no contact with children or with the soil. He is immunocompetent and otherwise healthy. He uses his hot tub several times a week and likes to take long, hot showers. Family medical history is negative for skin diseases of any kind. Examination shows approximately 20 round, uniformly and superficially scaly pinkish-brown papulosquamous lesions ranging from 1.0 to 2.8 cm on the patient's legs (shown), buttocks, and trunk. KOH examination of these lesions is negative. Elsewhere on his body, his skin is extremely dry, but his elbows, knees, nails, and scalp are otherwise normal in appearance • A) Nummular eczemaB) Tinea corporisC) PsoriasisD) Bowen's disease
A 24-year-old woman is referred to dermatology for evaluation of lesions that have been present on her face for three days. She reports several prior outbreaks of a similar nature, each of which lasted 10 to 12 days. The patient reports symptoms of tingling and itching, with a small amount of pain in the lesions -- symptoms that are identical to previous attacks. Although the patient has a history of chickenpox as a child -- and even though she feels fine -- her primary care provider initially made a diagnosis of chickenpox, then changed the diagnosis to shingles. Previous attacks were treated with a five-day course of valacyclovir, and the lesions gradually resolved, only to reappear later. The patient's medical history is unremarkable except for having atopic dermatitis. Examination shows the lesions to be discrete 3- to 5-mm vesicles, many with umbilicated centers, distributed evenly over the inferior one third of the face and upper neck. • A) Staph infectionB) Eczema herpeticum, or Kaposi's varicelliform eruptionC) VaricellaD) Molluscum contagiosum
For three weeks, a 22-year-old woman has had a rash, which has persisted over a good part of her body despite application of topical antifungal and steroid creams. She says that the rash started with one large, round, scaly lesion on her lower abdomen, followed within a day or two by the appearance of hundreds of smaller but similar lesions that are still manifesting after three weeks. The patient reports no other symptoms, but she is greatly concerned nonetheless. She denies fever and malaise and is otherwise healthy, and she has a monogamous relationship with her husband. On examination, the pinkish tan lesions are found to be papulosquamous, predominantly annular, with a curious fine scale in the center. They appear primarily on truncal skin, sparing the face, palms, soles, and lower legs. KOH examination of the scale is negative. • A) Pityriasis roseaB) Tinea versicolorC) Tinea corporisD) Secondary syphilis
A 40-year-old woman presents with a highly debilitating hand rash that started six weeks prior to this visit. She was referred by her primary care provider after he treated her with oral antibiotics (cephalexin 500 mg four times a day for 10 days) to no good effect. The patient is otherwise in good health, with no history of skin diseases or other serious illness. She has, however, been under more stress than she is accustomed to. The examination shows a bilateral palmar eruption characterized by discrete and coalescent pustules and erosions, producing raw skin in the central palm of both hands. There are no palpable nodes in either epitrochlear or axillary locations, and there is little if any redness around the rash. Examination elsewhere reveals a few 1- to 2-cm papulosquamous lesions on the legs; the patient reports that these appeared at about the same time as the palmar eruption. Moreover, there are pits in three of 10 fingernail plates, and a curious pink rash without scale in the upper intergluteal area. The feet are clear. • A) Chronic staph infectionB) Contact dermatitisC) PsoriasisD) Chronic fungal infection
A 45-year-old woman is referred to dermatology by her primary care provider for removal of cosmetically unacceptable lesions that have been present on her face, lips, neck, and arms for most of her life. She has been seen for them on a number of occasions, but the emphasis had always been on how to eliminate them rather than on determining their origin. The patient is otherwise healthy but has a family history of the lesions; a sibling has the same kind of lesions on her face, and her father, who also had an extensive history of gastrointestinal bleeds leading to a partial colectomy, had them as well. All three experienced excessive nosebleeds as children. The patient has no history of Raynaud's phenomenon or of esophageal complaints. Examination reveals a collection of blood-red papules and telangiectases on the tongue, cheeks, chin, neck, sclerae, and (to a lesser extent) the fingertips. These are obviously vascular in origin, being blanchable and nontender. The skin examination is otherwise normal • A) Dermatoheliosis (sun damage)B) Spider angiomasC) Hereditary hemorrhagic telangiectasiaD) CRST syndrome
A 14-year-old boy is brought in by his mother for evaluation of lesions present since age 6 months. The child is otherwise healthy and there is no history of skin disease in the family. The boy's pediatrician had suspected neurofibromatosis (NF), but since there was no family history of that malady and since the boy had not demonstrated any other signs of the disease, the decision had been made to wait and see what developed. But by now his mother is more concerned and has obtained a referral to dermatology. Examination reveals eight lesions ranging in size from 3 to 10 cm. They are roughly oval and are located on the trunk and in the axillary areas. They are macular and uniformly light tan. No other stigmata of NF are seen, but the patient is referred to an ophthalmologist, who confirms the diagnosis of neurofibromatosis type 1 (NF1) based on the presence of a particular lesion in the patient's iris. • The name of that lesion is: • A) Janeway's lesionB) Darier's signC) Gottron's papuleD) Lisch nodule • E. Café Au Lait spot
A 70-year-old woman presents for evaluation of a slightly sensitive erythematous patch of skin on her nose that has been present for more than a year. She reports that it has been slowly growing and that it is exacerbated by direct sun exposure. Because the lesion has persisted despite previous treatment for possible infection with oral and topical antibiotics and topical hydrocortisone 1% cream, her primary care provider referred her to dermatology. At this point, however, no medication has been applied to the lesion for months. The patient is otherwise healthy and has no joint pain, fever, or malaise. She is not diabetic, and there is no history of trauma to the area. No other skin lesions or conditions are noted on examination. The nose lesion is erythematous and nontender. It blanches with light pressure, and there is a faint amount of scale on its surface. There are no palpable nodes in the area • A 3-mm punch biopsy is performed, and it proves to be diagnostic. What is the most likely diagnosis? • A) Impetigo or other cutaneous bacterial infection • B) Discoid lupus erythematosus • C) Actinic keratosis • D) Contact dermatitis
A 4-mm punch biopsy is taken, which proves to be diagnostic. What is the most likely diagnosis? • Pityriasis rosea • Psoriasis • Dermatophytosis (tinea corporis) • Nummular eczema A 37-year-old businessman is referred to dermatology for the evaluation of round, scaly lesions that appeared suddenly three months previously, at around the same time his first child was born. The lesions, which are mostly asymptomatic, have been unresponsive to the application of over-the-counter antifungal creams (tolnaftate and clotrimazole). There are no pets in the house, and no one else in the household is similarly affected. Although he denies any history of skin problems, he believes his father had psoriasis. The patient does not smoke cigarettes, drink alcohol, or use prescription medications. He denies joint pain or swelling. Examination reveals a total of five round, uniformly scaly lesions on truncal and extensor extremity skin (a right anterior tibial lesion is pictured). They average about 2.5 cm in diameter. There is a salmon pink erythema in the background, and the scale is notably white and tenaciously attached to the underlying skin. Microscopic examination of scrapings from the periphery of two of the lesions (using a KOH preparation) is negative for fungal elements. Elsewhere on the patient's body, definite pits in four of 10 fingernail plates, scaly white plaques in the scalp, and scaling in both external auditory meatus are found. The patient's skin is not especially dry.
A 6-year-old boy is referred by his pediatrician to the dermatology department for evaluation and possible removal of a lesion. The lesion has been present since birth and has grown slowly with the child's growth. Initially thought to be a wart, it has persisted despite treatment with liquid nitrogen. The mother's main concern at this point is that her son's classmates are teasing him about the lesion. The child is otherwise healthy, and he is motivated to have the lesion removed. Examination reveals a linear 6 1-cm epidermal collection of brown, relatively dry, warty papules. Examination of the rest of the patient's skin reveals no other remarkable findings. • Epidermal nevus, congenital • Seborrheic keratosis • Wart • Congenital compound nevus
A 56-year-old woman presents with a lesion on the lateral aspect of her right foot. She reports that she first noticed it five years ago and that it has been slowly growing in size. Then, a few months ago, the lesion began to focally ulcerate. The patient consulted her primary care provider, who diagnosed the lesion as cellulitis and prescribed cephalexin. The lesion failed to respond, however, so the patient was referred to the dermatology department. The oddly pigmented, asymmetrical, 3-cm lesion is mostly macular, with focal areas of ulceration. It is not tender, red, or hot. The patient has red hair, fair skin, and blue eyes. She reports advanced sun damage from years of working as a lifeguard in Oklahoma. An incisional biopsy is performed, incorporating the darkest, most irregular portion of the lesion. The results are diagnostic. • Malignant melanoma, acral-lentiginous type • Birthmark (congenital nevus) • Wart • Persistent cellulitis
0.75 mm (comparable to Clark Level II) • > 0.75 - 1.5 mm (comparable to Clark Level III) • > 1.5 - 4.0 mm (comparable to Clark Level IV) • > 4.0 mm (comparable to Clark Level V) the overall five-year survival rate was 52 percent for patients with a primary melanoma of the foot or ankle compared to 84 percent for patients with melanoma on the thigh or calf.
A 40-year-old woman is seen in the dermatology clinic for evaluation of a "fungal infection" in her thumbnail. It has been present for six months -- despite an initial 10-day course of cephalexin and a two-month course of oral terbinafine, neither of which produced any change in the condition. The patient is nondiabetic, not immunosuppressed, and otherwise healthy. Her toenails are not involved, nor are any other fingernails. She reports that she is prone to vaginal yeast infections which occur for no apparent reason several times a year. Personal and family history of psoriasis is negative. Examination of the affected thumbnail reveals partial separation of the nail plate from the cuticle, a mildly dystrophic nail plate, modest edema, and scaling of the paronychial skin. Palpation of the latter is painful and produces a drop of pus, which is cultured. There are no rashes on her elbows or knees • A) Psoriatic nail disease • B) Bacterial infection • C) Squamous cell carcinoma • D) Chronic candidal paronychia • E) Onychomycosis (fungal infection)
68-year-old woman presents with an "infection" in her right arm that has been unresponsive to oral and parenteral antibiotics (cephalexin, ciprofloxacin, and vancomycin). The problem started four weeks earlier, with a small rash that she treated with topical antibiotic cream. The outbreak rapidly worsened and the patient consulted her primary care provider, who placed her on the oral antibiotics and, when that failed, admitted her to the hospital. The hospital's consulting infectious disease specialist obtains skin and blood cultures (neither showing any growth) and starts parenteral antibiotics, which yield no improvement. Since the patient's blood work results are unremarkable and she has no pain or fever, she is discharged and referred on an urgent basis to a dermatologist. More history taking reveals that the patient and her family have been applying a number of topical agents to the arm throughout the course of the episode, including a hydroxyquinoline sulfate salve and triple antibiotic cream. Examination reveals an afebrile patient in no distress. The dorsum of her right arm is bright red, with an extensive papulovesicular rash covering the entire extensor surface in a sharply demarcated pattern. Neither epitrochlear nor axillary nodes are palpable. The arm itself is not tender, but there is significant edema present. The volar surface of the arm is unaffected. • Bacterial infection • Herpes zoster • Bowen's disease (intraepidermal squamous cell carcinoma) • Contact dermatitis
A 35-year-old man presents complaining of bumps on his upper back that have slowly grown slightly larger. The patient reports that although they are not painful, one in particular frequently gets irritated from contact with clothing. He believes that they have been present for years; there are no lesions elsewhere on his body. The patient's medical history is remarkable for hypertension, which is well controlled with ramipril. His family medical history is unremarkable.
A 33-year-old man presents with an eruption of painful, itchy "blisters" on his hands and forearms evident for the past two days. There are no lesions elsewhere on his skin or mucous membranes. Contact history is negative, and the patient is taking no medications. He denies any previous eruptions.
A 29-year-old man presents for evaluation of changes in and around a mole on his face. He states that the mole has been present for as long as he can remember but in recent months has begun to "lose some color". The patient is particularly concerned because the skin surrounding the mole has also lightened in color. He has several other moles that have not changed. The patient's medical history and family medical history are unremarkable, and he is taking no medications.
A 14-year-old boy presents with a history of localized hair loss. His mother is not sure exactly how long this has been occurring: They may have noticed the patient's condition only because he is in the process of growing his hair to a longer style. She believes the area of hair loss may be slowly expanding. The patient admits to mild pruritus but is more concerned about teasing from his football teammates. His medical history is unremarkable, and he is taking no medications.
A 27-year-old man presents for treatment of "jock itch," which he states has been present for about six weeks. He has been using an over-the-counter powder marketed for this problem, without any result. He notes a prior history of athlete's foot, now resolved, and states that one of his teammates said the two conditions could be related. Past medical history is otherwise unremarkable. Physical examination reveals the lesions shown above but is otherwise unremarkable. There are no skin changes on the feet. KOH prep of the lesions above is positive; KOH prep of the interdigital spaces of the foot is negative
A 22-year-old man presents with an eruption on both forearms. He says that the eruption has been present for a week and has not responded to over-the-counter hydrocortisone cream (0.5%). The eruption is intensely pruritic, and the patient scratches the affected area almost continuously during your interview. Past medical history reveals problems with chronic diarrhea (for which he is currently being worked up) and bipolar disorder. He is currently taking loperamide and lithium (his lithium level is within therapeutic range). The patient is employed by a lawn maintenance service
A 65-year-old man presents for a routine physical examination. There are several sharply demarcated, hyperpigmented macules on his shoulders, neck, and forearms. The patient reports increasing numbers of these macules in recent years but no symptoms associated with them. The lesions are nonscaling and have distinct margins and relatively uniform color, although some show intralesional pigment variation. The patient is currently taking atorvastatin calcium for hyperlipidemia; his medical history is otherwise unremarkable.
A 33-year-old woman presents for a pruritic eruption on her lower left shin that has been present and worsening for two to three months. She is employed as a systems analyst. The patient is taking no medications. She has a negative contact history and an unremarkable medical history and review of systems. Examination reveals an eruption, confined to a single location, involving epidermal thickening and excoriation.
A 48-year-old woman presents for evaluation of "moles" on her eyelids. She states they have been present for several months and are slowly enlarging. She denies any associated symptoms such as pruritus, pain, or bleeding and has noted no other similar lesions. Past medical history is remarkable for hysterosalpingo-oophorectomy at age 45 years for fibroids, and she is currently receiving hormone replacement therapy. Family medical history is remarkable for coronary artery disease in her father and one brother.
A 23-year-old man presents for a persistent, slowly worsening rash to the face. He states that it first occurred in January; it is now March. He denies any pruritus. He has experienced some relief with over-the-counter 0.5% topical hydrocortisone. The patient has tried changing soaps and shampoos without effect. He notes a fair amount of cosmetically unacceptable scale, including the scalp area, which he has been attempting to wash off. Past medical history and review of systems are unremarkable, and the patient is using no medications.
A 67-year-old man presents with a complaint of worsening "eczema." He states that he has a long history of eczema, with eruptions that worsen somewhat in the winter months. However, this current eruption on the trunk and extremities is more severe and pruitic than he has ever experienced. It has been present for about 10 days and has not responded to increased oral hydration, topical moisturizers, or topical corticosteroids. Past medical history is remarkable for episodic gout, for which he began allopurinol therapy last m
A 40-year-old man presents for treatment of "athlete's foot." He has a history of recurrences, which in the past have responded well to prescribed or over-the-counter topical antifungal agents. His current pruritic eruption has been gradually worsening for several weeks despite the use of topical clotrimazole. He has no other significant positive medical history. Examination reveals the eruption shown. The plantar surfaces and interdigital spaces are unremarkable, and KOH prep is negative.