Download
1 / 58
760 likes | 2.34k Views
CANDIDIASIS. CONTENTS. Introduction Candida albicans Predisposing factors Pathophysiology Classification Clinical features Lab diagnosis Treatment. Introduction. Candidiasis is caused by a yeast-like fungus- Candida Albicans

E N D
CONTENTS • Introduction • Candida albicans • Predisposing factors • Pathophysiology • Classification • Clinical features • Lab diagnosis • Treatment
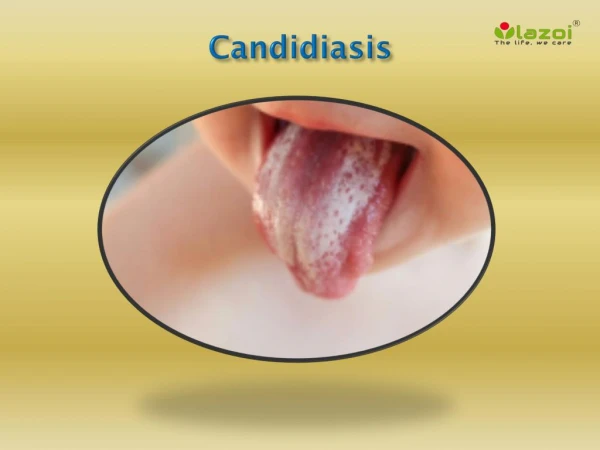
Introduction • Candidiasis is caused by a yeast-like fungus- Candida Albicans • French Pediatrician- FrancosisValleix (1838) • Candida- Latin word (white) • Synonyms Candidosis Moniliasis Thrush
candida • The genus candida is a collection of 150 Asporogenous yeast species • 7 candida species are of major medical importance C. albicans, C. tropicalis, C. Krusei, C. lusitaniae, C.dubliniensis and C. Parapsil
Candida Albicans • 3 forms A.Yeast cells B.Truehyphae & Pseudohyphae C.Chlamydospores • CONDITIONS CONDUCIVE Temp- 20-40ᵒc Ph range 2-8
A.Yeast cell • Temp- Below 33ᵒc • Ovoid (3-5µm) • Bud formation occurs preferentially at polar region of the cell
The presence of a suitable nitrogen source during the starvation period primes the yeast cells for morphogenesis & allows glucose ammonium ions to act as the inducers
Germ tube • Near neutral ph mycelial growth is favored • Conversion of a yeast cell to a hyphal cell occurs – Germ tube formation • Multiple protuberances arise in the early stage • Only one germ tubes develop- True hyphal cell
Pseudohyphae are long branching filaments of elongated yeast cells formed by polar budding & constricted at the site of emergence with a septum • Calcofluor white stained Candida albicans showing true hyphae (*) and pseudohyphae (+).
C. albicans is a relatively common inhabitant of the oral cavity • thus presence of the fungus is not sufficient to produce the disease- opportunistic pathogen • Predisposing factors local systemic
Pathophysiology ( candida virulence factors) • Adherence of Candida to human epithelial cells is initiated through weak and reversible interactions involving hydrophobic and electrostatic forces . • Specific adhesion between Candida and receptors on host tissues results in a stronger covalent attachment • Candida genes of the ALS (agglutinin-like sequence) family and also HWP1 (hyphal wall protein) encodes - promote adhesion of C. albicans to epithelial surfaces.
Specific interaction of Candida with oral bacteria has also been demonstrated that could encourage biofilm formation on dentures and in dental plaque • The pathogenic significance of being able to produce hyphae could relate to the greater resistance of hyphae to phagocytosis compared with yeast, • the ability of hyphae to invade epithelial layers resulting in tissue damage
Candida produces several extracellular enzymes that could have a locally damaging effect on host structures Aspartylproteinases (SAPs) – Promoting hyphal growth • Albicansproteinases- facilitate initial penetration of keratinised cells- keratinolytic activity
The white plaque of candidiasis are produced by invasion of the epithelium by candidialhyphae & a proliferative epithelial response • The texture of the plaque – Infiltration of the epithelium by inflammatory exudate • Neutrophils are concentrated particularly at the junction with the glycogen rich zone – microabscesses • A line of weakness is thus produced at the base of the plaque , enabling it to be readily wiped off
Oral candidiasis WHITE ACUTE HYPERPLASTIC& ATROPHIC CHRONIC RED
classification • Most adopted classification proposed by Lehner (1966)
Proposed revised classification of Oral candidiasis Acute forms(Samaranayake ,1991 and modified by Axell et al,1997) • Pseudomembranous • Erythematous. Chronic types • Hyperplastic • Nodular • Plaque-like • Erythematous • Pseudomembranous Candida-associated lesions • Angular cheilitis. • Denture stomatitis. • Median rhomboid glossitis.
Keratinized primary lesions superinfected with Candida • Leukoplakia. • Lichen planus. • Lupus erythematosus Secondary candidosis • Oral manifestations of systemic mucocutaneouscandidosis as a result of diseases such as thymicaplasia and candidosisendocrinopathy syndrome
Pseudomembranouscandidiasis(Thrush) • Most frequently encountered form of the disease. • May occur at any age but is especially prone to occur in debilitated or chronically ill elderly pts or in infants • Site- bucall mucosa, tongue but also seen on the palate, gingiva,& floor of the mouth.
Clinical Features • Semi-adherent, whitish, yellowish, soft and creamy, slightly elevated, pseudomembranous, drop-like or confluent patches or plaques, resembling milk curds.
Plaques can be easily removed by wiping with a gauze swab, leaving a red and slightly bleeding surface or even a shallow ulceration. • The clinical sign is useful in distinguishing acute pseudomembranous from leukoplakia which by definition cannot be rubbed off. • Lesions may be localized or may involve the entire oral mucosa.
ERYTHEMATOUS CANDIDASIS • Erythemaouscandidiasis may be termed acute or chronic. • The acute form was formerly known as acute atrophic candidiasis • Condition may be associated with angular cheilitis
Erythematouscandidiasis also known as “Antibiotic sore mouth” • Characterised by central papillary atrophy of tongue • As a sequelae to a course of broad spectrum antibiotics, corticosteroids or any disease which supress the immune system-HIV
D/D • Erythroplakia Borders are sharp & well demarcated
Chronic hyperplasticcandidiasis(candidalleukoplakia) • White patch that cannot be removed by scraping • Occurs bilaterally in comissural regions of buccal mucosa • Highest prevelence in middle aged men who are smokers • Least common
Some investigators believe that this condition simply represents candidasis that is superimposed on a preexisting leukoplakia lesion, a situation that may certainly exist at times.
Few keratotic lesions which may be superimposed by candidial infection Leukoplakia Lichen planus Lupus erythematous
Candida Associated lesionsCandida Associated Denture Stomatitis • 65% of Denture wearers • Asymptomatic • Cause; Ill fitting dentures Limited flow of saliva Dentures where not adequately cleansed or is retained overnight in the oral cavity
Under these conditions the stagnant area above the upper fitting surface of the denture provides an ideal environment for the growth of candida • Candida adept to denture by adhering to acrylic used as the base material for the denture
ANGULAR CHEILITIS: (PERLECHE, ANGULAR STOMATITIS) • Tenderness, erythema and fissuring of the corners of the mouth. • It can affect one or both corners of the mouth. • Commissures appear wrinkled and with time deep fissures develop with a tendency to bleed. • As mixed bacterial/fungal aetiology.
Poor dentures with inadequate vertical component allowing the skin at the commissures to crease and accentuated folds at the corners of the mouth. saliva tends to pool in these areas, keeping them moist and thus favoring a yeast infection
AIDS –RELATED ORAL CANDIDIASIS • Oropharyngealcandidiasis - most common opportunistic infection observed in AIDS patients, occurring in an estimated 80 to 95% of these patients, when the CD4 T-lymphocyte counts are below 200 cells/mm3. Oral candidiasis may appear as : • Pseudomembranous • Erythematous • Hyperplaslic • Angular cheilitis.
MEDIAN RHOMBOID GLOSSITIS (MRG) • MRG has been regarded as a failure of withdrawal of the tuberculumimpar during the development of tongue. • The absolute lack of cases of MRG in newborns and other infants • variant form of erythematouscandidiasis. Most recent authors have subscribed to this theory that MRG is an acquired chronic oral candidasis; found frequently in patients with denture stomatitis.
Diagnosis • The diagnosis of candidiasis is usually established by the clinical signs, along with exfoliativecytologic examination
LABORATORY DIAGNOSIS OF CANDIDA Classic sampling methods • Smear • Swab • Biopsy OtherMethods • Imprint culture • Collection of whole saliva • The concentrated oral rinse • Impression culture technique
Smear/ biopsy • Periodic acid-Schiff (PAS) method: • Candidalhyphae & yeast can be identified • Stains the carbohydrate present in abundance in the cell walls, making the organisms bright magenta in color. • To make diagnosis, one must be able to see hyphae & pseudohyphae. • Hyphae are 2µm in diameter, vary in length & may show branching.
KOH • 10-20% KOH preparation may be used for rapid evaluation. • KOH lyses the background of epithelial cells, allowing more resistant hyphae to be visualized. • disadvantages; lack of a permanent record less staining of fungal organisms compared to PAS Inability to assess the nature of the epithelial cells
Biopsy; • Depending on clinical form, the histological featues vary. • Common features include increased thickness of parakeratin with elongation of rete ridges. • Chronic inflammatory infiltrate may be seen in connective tissue immediately subjacent to infected epithelium.
Small collections of neutrophils (microabscesses) often identified in parakeratin & superficial spinous layer near organisms. • Hyphaeembedded in the parakeratin layer & rarely penetrate into viable cell layers unless patient extremely immunocompromised
Superimposed candidiasis on premalignant condition will be at an increased risk of malignant change • It often induces hyperplasia & a degree of cytological atypia
Stains used are; Grocott- Gomorismethanamin silver Gridley’s stain Calcoflour white stain
Culture Media • The most frequently used primary isolation medium for Candida is SABOURAUD DEXTROSE AGAR (SDA) with antibacterial antibiotics and incubated at 37°C. • candida develops as cream, smooth, pasty convex colonies on SDA and differentiation between species is rarely possible.
In recent years, differential media have been developed that allow identification of certain Candida species • based on colony appearance and colour following primary culture Advantages: the presence of multiple Candida species in a single infection can be determined which can be important in selecting subsequent treatment options
Pagano-Levin agar CHROMagarCandida-identifies C. albicans, C. tropicalis, and C. krusei, C. dubliniensis Albicans ID Fluroplate, or Candichromalbicans
Identification of yeasts based on primary culture media can be confirmed through a variety of supplemental tests- GERM-TUBE TEST