Download
1 / 88
880 likes | 1.07k Views
Comprehensive Pain Mangement: Beyond F-Tag 309. Debra Bakerjian PhD, RN, FNP President and CEO, geriHEALTHsolutions Chair, Clinical Advisory Workgroup, Advancing Excellence Postdoctoral Fellow, University of CA, Davis Assistant Adjunct Professor, University of CA, San Francisco. Objectives.

E N D
Comprehensive Pain Mangement:Beyond F-Tag 309 Debra Bakerjian PhD, RN, FNP President and CEO, geriHEALTHsolutions Chair, Clinical Advisory Workgroup, Advancing Excellence Postdoctoral Fellow, University of CA, Davis Assistant Adjunct Professor, University of CA, San Francisco
Objectives • Recognize specific strategies to improve pain management • Identify best-practice resources to improve pain care for nursing home residents • Learn how to access resources and set goals on the Advancing Excellence web site and the Geriatric Pain web site to manage pain • Understand the regulatory requirements for pain management in NHs –Ftag 309
The Problem • Pain is under-recognized and undertreated • The prevalence of pain is reported as high as 85% in NHs • Some reported improvement in prevalence of pain • Over 75,000 long stay residents have mod-severe pain • Ove 150,000 short stay residents with mod-severe pain
Solution • Develop systemized approach to pain management • Consists of “program of care” • Requires ongoing evaluation and refinement • Program based on “evidence based care” and “best practices” in pain management
The Intent of Quality of Care Regulatory Guidelines “Each resident must receive and the facility must provide the necessary care and services to attain or maintain the highest practicable physical, mental, and psychosocial well-being, in accordance with the comprehensive assessment and plan of care. “
What is F-tag 309? • F-tag 309 focus is overall quality of care – much of the f-tag has not changed • Requires that NHs provide for the highest practicable level of function & well being • Comprehensive resident assessment • Care plans must address mental, physical, & psychosocial needs • Ensure residents obtain optimal improvement or do not deteriorate • Within resident’s right to refuse • Limits of recognized pathophysiology & normal aging
New Aspects of F-tag 309 • Revised general investigative protocol • Any QOC issue not covered specifically by another F-tag is covered here • Added Hospice guidelines • Added dialysis guidelines • Removed unintended weight loss – now in F tag 325
New Pain Aspects of F-tag 309 • Pain management has specifically developed guidelines within this F-tag • New definitions of terms • New investigative protocol • Defining care processes for pain management • Defined steps in pain recognition, assessment, management, interventions, care plans • Investigative protocol for surveyors specific to pain
Definition of Terms • Addiction • Adverse consequence, adverse drug reaction • Adjuvant analgesics • Complimentary and Alternative Medicine (CAM) • Non-pharmacological interventions • 4 types of pain – acute, breakthrough, incident, persistent or chronic • Physical dependence • Standards of practice • Tolerance
Overview of Pain Recognition & Management • Facilities & staff must be committed to effective pain management • Pain can be acute or chronic & staff must evaluate resident reports of pain or nonverbal signs of pain • Residents with cognitive impairment must also have their pain recognized & managed • Facilities must break down myths about pain in older adults • Staff, resident & family misperceptions about effective pain management
Care Processes for Pain Management • Assess for potential for pain • Recognize the onset or presence of pain • Address & treat underlying cause for pain • Develop & implement pain interventions • Identify & use specific strategies for different levels or sources of pain • Monitor appropriately • Modify pain interventions/strategies as needed
Pain Recognition • All staff are responsible for recognizing pain upon admission and throughout the stay • Recognition efforts must go beyond asking the question “are you in pain” • Verbalizations may be nonsensical • Non-verbal indicators • Aberrant behaviors • Functional decline • Loss of appetite • Difficulty sleeping • Observations should be at rest & with movement
Assessment • Observing during care, activities & treatments can detect presence of pain, location, & limitations on residents • MDS must be completed as “part” of the comprehensive assessment • Facilities must document a more detailed assessment that identifies problem, needs, monitors condition, records treatment & response to treatment
Pain Assessment Standards • History of pain & its treatment • Characteristics of pain • Impact of pain on quality of life • Factors that precipitate pain • Strategies or factors that reduce pain • Associated pain symptoms • Physical examination • Current medical condition & medications • Resident goals for pain management
Management of Pain • Based on assessment, facility, attending prescriber, staff collaborate to manage pain • Develop appropriate interventions to prevent or manage pain • Interventions may be integrated into care plan or included as a specific pain management need or goal • IDT & resident develop pertinent, realistic & measurable goals for treatment • Pain management approaches must follow clinical standards of practice
Non-Pharmacological Interventions • Alterations in environment for comfort • Physical modalities – cold/heat, positioning • Exercises to reduce stiffness, prevent contractures • Cognitive/behavioral interventions • CAM – herbal supplements if ordered
Pharmacological Interventions • IDT is responsible for developing individualized pain management regimen • A systematic approach for meds and doses is important • Addressing underlying cause of pain • Administration timing – PRN vs routinely • Combining short & long acting • All medications including opioids or other potent analgesics must be dosed according to standards • Clinical record should reflect ongoing communication with prescriber
Monitoring, Reassessment, Care Plan Revision • Monitoring response over time helps to determine effectiveness of treatments • Adverse consequences to medications can be anticipated & reduced • Identification of target signs of pain • Inadequate control of pain requires a revision of intervention • Resolution of pain should be documented and treatment tapered or discontinued
Investigative Protocol • QOC related to recognition & management of pain • Determine whether facility has provided & resident has received care & services to address & manage pain • Applies to residents who state they have pain, who display indicators of pain, are assessed with pain, receives pain treatment, has elected hospice benefit for pain management
Survey Procedures • Observe residents • Interview residents or family • Interview nurse aides • Review records • Assessment • Care plan, including revisions • Interview health care practitioners & other health professionals
Determining Compliance • Facility is in compliance if EACH resident has their pain managed in alignment with their goals to attain the highest practicable physical, mental, & psychosocial well-being • Recognize, evaluate pain to determine cause • Developed & implemented comprehensive care plan • Provided measures to minimize, prevent, or treat pain • Monitor effects of interventions • Communicate with health care practitioner when appropriate to obtain new orders or revise current orders
Noncompliance Determination • Failure to show adequate proof that ALL of the previous steps are followed is non-compliance • Non-compliance can be at any one step along the way • Recognize & evaluate • Intervene & treat • Prevent or minimize • Monitor • Communicate & coordinate
Related or Associated F-tags • F155 – Right to refuse treatment • Facility must assess reason, clarify & educate resident of consequences, offered alternatives & documented these steps • F157 – Notification of changes • Health care practitioner notified if pain persisted or there were adverse consequences • Notified responsible party of changes • F242 – Self-determination & participation • Facility provided resident with relevant options to manage pain
Related or Associated F-tags • F246 – Accommodation of needs • Adopted resident’s physical environment to reasonably accommodate resident’s pain • F272 – Comprehensive assessments • Was a comprehensive assessment done • F278 – Accuracy of assessments • Does the assessment reflect the resident’s condition
Related or Associated F-tags • F279 – Comprehensive care plan • Did care plan include measureable objectives, time frames, & specific interventions/services • Was it consistent with resident’s risks, needs, goals, preferences, & current standards of practice • F280 – Comprehensive care plan revision • Ensure periodic review of plan & revision as needed by qualified TEAM with input from resident or responsible party
Related or Associated F-tags • F281 – Services meet professional standards of quality • F282 – Care provided by qualified person in accordance with plan of care • F329 – Unececessary drugs • Are medications monitored for effectiveness & adverse consequences • Are symptoms resident has related to meds
Related or Associated F-tags • F385 – Physician supervision • Is pain management supervised by physician, including participation in comprehensive assessment process, development of treatment regimen, monitoring & response to notification of changes in resident status • F425 – Pharmacy services • Were medications available & administered as indicated, ordered at admission & throughout stay
Related or Associated F-tags • F501 – Medical Director • Did Medical Director help develop & implement appropriate policies c/w standards of practice • Did Med Director interact with resident’s physician supervising the care if requested by facility • F514 – Clinical records • Did clinical records accurately & completely document resident status, care/services provided, in accordance with standards & resident goals • Did records provide a basis for determining & managing resident progress & responses to care
Knowledge of Pain • Know principles of pain management • Types of pain & pain terminology • How to perform a comprehensive assessment • Correct documentation of findings • Understand both pharmacological & non-pharmacological interventions • How to monitor & revise plans • Effective communication
Pain Principles • Pain is under-recognized & undertreated • Older adults have the right to have pain assessed & treated in accordance with their goals for pain management • Pain is subjective- self-report of pain is most reliable indicator • Physiological & behavioral signs are neither sensitive nor specific & can’t replace self-report • Assessment tools & treatments need to be appropriate & individualized each resident • Pain tolerance varies & is individual • Prevent &/or manage medication side effects • Worry about addiction to opioids is not a credible reason for withholding opioid pain medication
Pain Terminology • Pain characteristics are used to describe pain • Duration – how long pain has been present • Frequency – number of occurrences in a given time period • Intensity – descriptive rating based on scale • Location – anatomic site • Onset – how does pain start • Pattern – how does pain vary throughout the day, what affects pain – makes it worse or better • Quality – use the resident’s description; provide examples such as aching, cramping, sharp, throbbing, dull, sharp, burning, radiating, shooting
Pain Recognition • Staff must recognize pain or potential pain • All staff are responsible for helping with pain management • Therapy • Activities • Social services • Pharmacy consultants • Staff must act on their observations • All staff must be educated to recognize pain • Once staff know individual resident triggers – all staff must be told about what to observe
Indicators of Pain • Verbal indicators – words & vocalizations • Written indicators – written interpretations in native languages, written notes from residents • Non-verbal indicators – facial expressions, behavioral abnormalities, fidgeting, withdrawal, non-movement
Comprehensive Assessment • All residents must have comprehensive pain assessment upon admission • Residents who trigger for pain (through MDS/RAI) or have diagnosis of chronic pain or exhibit frequent pain must have comprehensive pain assessment • Most pain experts recommend weekly assessments
Comprehensive Assessment • Should be appropriate based on cognitive status • If resident cognitively intact – use verbal descriptors in their words to describe the pain • If cognitively impaired – use a screening tools • PACSLAC – screens for behaviors that may be pain related • PAINAD – monitor directly observable behaviors in adults with chronic pain • Comprehensive includes history descriptions, functional status & physical exam • Evaluate of impact on pain on ADLs, sleep, other functional activities
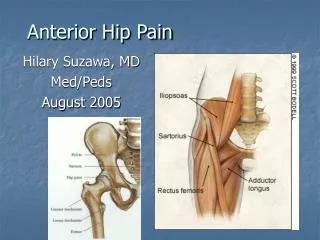
Major Categories of Pain Neuropathic • Source: peripheral nerve or CNS pathology • Examples: postherpetic neuralgia, diabetic neuropathy, spinal stenosis • Character: shooting, burning, electric shock, tingling • Requires different types of medications than nociceptive pain Nociceptive • Sources: organs, bone, joint, muscle, skin, connective tissue • Examples: arthritis, tumors, gall stones, muscle strain • Character: dull, aching, pressure, tender • Responds to traditional pain medicines & therapies
Documentation & Reporting • Forms should include resident goal, pain characteristics, history, & physical exam related to location & causes of pain • Ex. If pain in abd – check for bowel sounds, pain with palpation • If pain in leg – observe the site & look for s/sx trauma • Report to MD, NP or PA & other nurses should be complete but concise • Be sure to include CNAs in reporting & care planning
Principles of Pain Management • Should be individualized & match the need • Chronic pain should be treated with long-acting medications routinely • Breakthrough pain should be treated with short acting meds with rapid onset • Treat with lowest strength med to achieve pain control based on resident goals • Minimize side effects & adverse effects
Managing Pain • Frequent reassessment of resident & review of care plan • Determine what works & what doesn’t work • Discontinue what doesn’t work • Revise care plan to try new interventions • Collaborate with IDT & resident/family • Try new things or new ways such as changing the timing or dosing of medications
Non-pharmacologic Interventions • Traditional • Positioning • Massage • Environmental – lighting, room temperature, noise • Heat and/or cold applications • Diversion – social interaction • CAM • Now recognized as a part of therapy • May involve herbals & that must be communicated
Medication Management • Non-opioid • Opioids – mild to moderate • Opioids – moderate to severe • Repositioning • Heat and Cold • Breathing & Guided Imagery • Distraction • Massage • Music • Relaxation Pharmacological Non-Pharmacological
Pharmacologic Interventions • Non-opioids • Tylenol • NSAIDs such as Ibuprofen • Side effects in older adults (damage to kidneys, GI bleed) • Opioids • Types of opioids, routes of administration • Length of action • Side effects – constipation, confusion • Adjuvant therapy • Muscle relaxants • Seizure meds for neuropathic pain
Managing Side Effects • Most pain meds have potential side effects, particularly opioids • Side effects need to be anticipated and managed • Common opioid side effects include • Drowsiness • Respiratory depression • Constipation • Nausea • Delirium – particularly in residents > 85 yrs • Itching
Managing Side Effects • Side effect management should be part of the care plan • Side effect treatments need to be individualized • Reduced dosages • Alternate opioid • Bowel regimens • Medications to treat side effect if necessary • Obtain appropriate orders from prescribers • Care plan effective management techniques
Resident Centered Care Plan • Includes residents goal for pain management • I want my pain relieved so I can sleep • I want pain treatment before my therapy • I would like my pain reduced to level 4-5 • Care plan should include both drug and non-drug interventions • Care plan should include managing side-effects, decreased respirations,
Effective Communication • Nurses need to be able to understand resident pain issues and to use the right language in describing • Pain related problems need to be effectively communicated to prescribers • Pain related issues need to be documented accurately using appropriate language