Download
1 / 1
10 likes | 169 Views
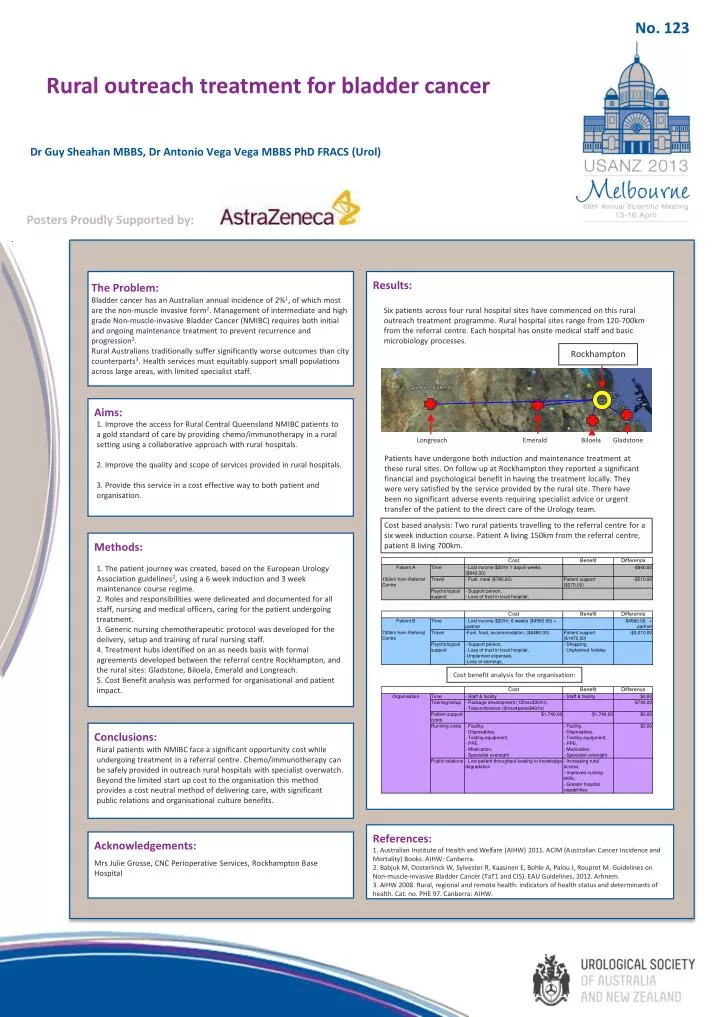
Rockhampton. Longreach. Emerald. Biloela. Gladstone. Cost based analysis: Two rural patients travelling to the referral centre for a six week induction course. Patient A living 150km from the referral centre, patient B living 700km. Cost benefit analysis for the organisation:. No. 123.

E N D
Rockhampton Longreach Emerald Biloela Gladstone Cost based analysis: Two rural patients travelling to the referral centre for a six week induction course. Patient A living 150km from the referral centre, patient B living 700km. Cost benefit analysis for the organisation: No. 123 Rural outreach treatment for bladder cancer Dr Guy Sheahan MBBS, Dr Antonio Vega Vega MBBS PhD FRACS (Urol) Posters Proudly Supported by: Results: The Problem: Bladder cancer has an Australian annual incidence of 2%1, of which most are the non-muscle invasive form2. Management of intermediate and high grade Non-muscle-invasive Bladder Cancer (NMIBC) requires both initial and ongoing maintenance treatment to prevent recurrence and progression2. Rural Australians traditionally suffer significantly worse outcomes than city counterparts3. Health services must equitably support small populations across large areas, with limited specialist staff. Six patients across four rural hospital sites have commenced on this rural outreach treatment programme. Rural hospital sites range from 120-700km from the referral centre. Each hospital has onsite medical staff and basic microbiology processes. Aims: 1. Improve the access for Rural Central Queensland NMIBC patients to a gold standard of care by providing chemo/immunotherapy in a rural setting using a collaborative approach with rural hospitals. 2. Improve the quality and scope of services provided in rural hospitals. 3. Provide this service in a cost effective way to both patient and organisation. Patients have undergone both induction and maintenance treatment at these rural sites. On follow up at Rockhampton they reported a significant financial and psychological benefit in having the treatment locally. They were very satisfied by the service provided by the rural site. There have been no significant adverse events requiring specialist advice or urgent transfer of the patient to the direct care of the Urology team. Methods: 1. The patient journey was created, based on the European Urology Association guidelines2, using a 6 week induction and 3 week maintenance course regime. 2. Roles and responsibilities were delineated and documented for all staff, nursing and medical officers, caring for the patient undergoing treatment. 3. Generic nursing chemotherapeutic protocol was developed for the delivery, setup and training of rural nursing staff. 4. Treatment hubs identified on an as needs basis with formal agreements developed between the referral centre Rockhampton, and the rural sites: Gladstone, Biloela, Emerald and Longreach. 5. Cost Benefit analysis was performed for organisational and patient impact. Conclusions: Rural patients with NMIBC face a significant opportunity cost while undergoing treatment in a referral centre. Chemo/immunotherapy can be safely provided in outreach rural hospitals with specialist overwatch. Beyond the limited start up cost to the organisation this method provides a cost neutral method of delivering care, with significant public relations and organisational culture benefits. References: 1. Australian Institute of Health and Welfare (AIHW) 2011. ACIM (Australian Cancer Incidence and Mortality) Books. AIHW: Canberra. 2. Babjuk M, Oosterlinck W, Sylvester R, Kaasinen E, Bohle A, Palou J, Roupret M. Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and CIS). EAU Guidelines, 2012. Arhnem. 3. AIHW 2008. Rural, regional and remote health: indicators of health status and determinants of health. Cat. no. PHE 97. Canberra: AIHW. Acknowledgements: Mrs Julie Grosse, CNC Perioperative Services, Rockhampton Base Hospital