Download
1 / 10
100 likes | 224 Views
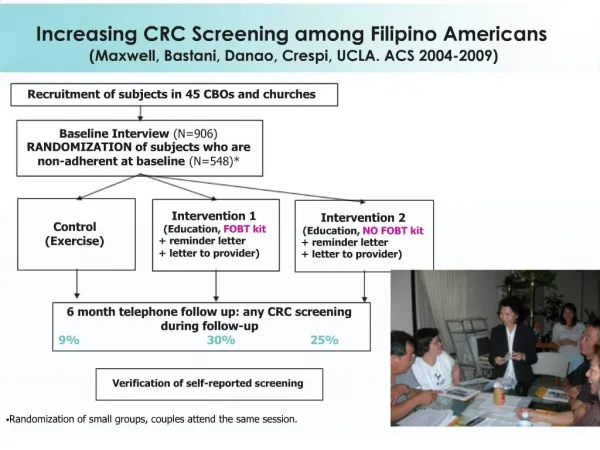
Increasing CRC Screening among Filipino Americans (Maxwell, Bastani, Danao, Crespi, UCLA. ACS 2004-2009). Recruitment of subjects in 45 CBOs and churches. Baseline Interview (N=906) RANDOMIZATION of subjects who are non-adherent at baseline (N=548)*. Control (Exercise).

E N D
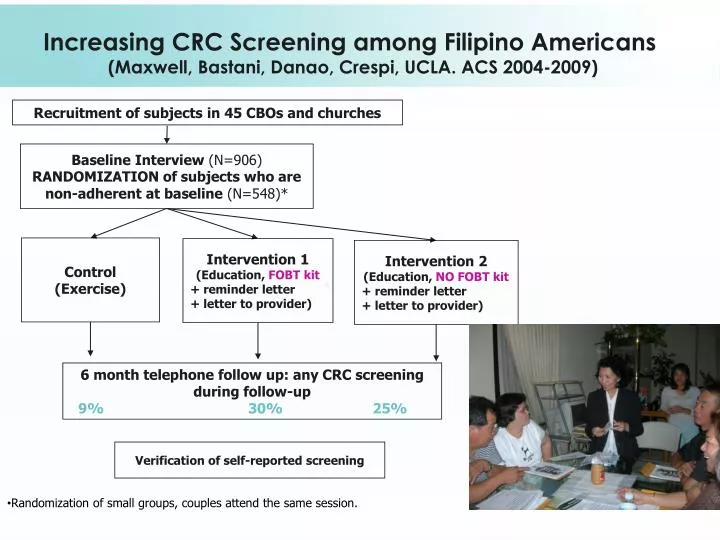
Increasing CRC Screening among Filipino Americans (Maxwell, Bastani, Danao, Crespi, UCLA. ACS 2004-2009) Recruitment of subjects in 45 CBOs and churches Baseline Interview (N=906) RANDOMIZATION of subjects who are non-adherent at baseline (N=548)* Control (Exercise) Intervention 1 (Education, FOBT kit + reminder letter + letter to provider) Intervention 2 (Education, NO FOBT kit + reminder letter + letter to provider) 6 month telephone follow up: any CRC screening during follow-up 9%30%25% Verification of self-reported screening • Randomization of small groups, couples attend the same session.
Estimates of the efficacy of the intervention NPV, negative predictive value; PPV, positive predictive value. * Maxwell AE, Bastani R et al. American Journal of Public Health 2010.
Efficacy of combinations of intervention components Analyses included all participants who attended a small-group session and provided sufficient information to enable a letter to be mailed to their provider. Adjusted for baseline differences, PPV and NPV of self-report. * evidence-based intervention strategies
Group-randomized design (as funded) 10 CBOs Randomize 5 CBOs Basic Dissemination (one-time training of CHAs & distribution of materials) 5 CBOs Organizational Dissemination (basic dissemination + workshop with CBO leaders to implement 5 organizational changes to promote CRC screening + 6 booster sessions/year with CHAs) 5 CBOs x 5 CHAs x 8 subjects = 200 subjects 5 CBOs x 5 CHAs x 12 subjects = 300 subjects Community Dissemination of an Evidence-based CRC Screening Intervention (Maxwell, Bastani, Danao, Crespi, UCLA. ACS 2010 – 2014) CHA = Community Health Advisor Assessments: Telephone interviews of subjects, organizational assessments, health advisor debriefings and log sheets.
Organizational changes Actions Targeting CBOs Changes in change agents Develop community capacity Community awareness of issue Health Care Environment Insurance status Filipino American Community Changes in health Health care providers Changes in risk factors and protective factors Filipino CBOs The Racial and Ethnic Approaches to Community Health (REACH) Model of Change Question: Include only orgs from CRC1 Study, new orgs or both? Centers of Disease Control and Prevention, adapted from Hill et al., 2007.
Research Question: What strategy to disseminate a CRC screening intervention has the greatest impact when administered in Filipino American community settings? Evaluation Framework: RE-AIM • REACH: CHAs in the organizational dissemination arm will disseminate CRC screening to more subjects than CHAs in the basic dissemination arm. • EFFECTIVENESS: Filipino Americans in the organizational dissemination arm will exhibit higher screeningrates at 6 mos follow-up than those in the basic dissemination arm. • ADOPTION: Organizational dissemination will result in better organizational adoption of activities to promote CRC screening compared to basic dissemination. • IMPLEMENTATION: Given technical assistance and resources, CBOs can implementevidence-based strategies to promote CRC screening among Filipino Americans. • MAINTENANCE: Organizational dissemination will result in better maintenance of activities to promote CRC screening compared to basic dissemination. Question: what constitutes Maintenance? No more technical and financial support for orgs? How do we assess Maintenance activities without influencing organizations and CHAs? When does Maintenance phase start in the basic and organizational dissemination arm?
RE-AIM Measures • Reach: # of subjects enrolled, how do enrolled subjects compare to the larger FA population? Compare refusals & participants, drop-outs & completers • Effectiveness: # of subjects screened at 6 months • Adoption: # of dissemination activities conducted per month and per subject in year 2. • Implementation: compare activities reported by CHAs and subjects to protocols. • Maintenance: # of dissemination activities conducted per month and subject in years 3 to 4.
NCCDPHP Knowledge to Action Framework Translation Phase Inst. Phase ResearchPhase Discovery Practice-based Discovery Efficacy Practice-based Evidence Effectiveness and Implementation Dissemination Decision to Adopt Knowledge to Products Practice Institution-alization Decision to Translate Engagement Diffusion Supporting Structures Supporting Structures Supporting Structures Evaluation Question: Can a 4 year study really assess all components from effectiveness to institutionalization?
Individual & Setting Level Predictors of Implementation Question: Are there existing measures we can use to assess these variables? Which variables are most important? Relationship Length of relationship, credibility, trust Relationship Position of CHA within org Graphic developed from article by Rabin, Nehl, Elliot, Deshpande, Brownson, Glanz. Implementation Science 2010
Discussion Questions • Importance of community awareness: Conduct the trial with “veteran” or “virgin” organizations or both? • Criteria for selection & randomization of orgs (size of membership, SES of geographic area in which org is located, church versus non-faith based orgs) • Basic dissemination arm: how can we conduct frequent assessments without contaminating this arm • Maintenance phase - when does it start: after 2 years of implementation? - continue to provide financial support to orgs during maintenance phase? - limit assessments to one exit interview to not influence level of activities during the maintenance phase? • Assessment What are the main organizational and CHA variables that we should assess? How to deal with organizations that are dropping out? • Contribution to Dissemination & Implementation Science How can our data inform the Model of Change and RE-AIM?