Download
1 / 20
200 likes | 355 Views
Barriers and Facilitators to CRC Screening in Southwestern Native Americans. Navajo Nation Human Research Review Board Conference November 16, 2011 Christina Getrich , PhD Robert Rhyne , MD. Funded by NIH-NCI Grant 5R21CA121066.

E N D
Barriers and Facilitators to CRC Screening in Southwestern Native Americans Navajo Nation Human Research Review Board Conference November 16, 2011 Christina Getrich, PhD Robert Rhyne, MD Funded by NIH-NCI Grant 5R21CA121066
Background • National incidence rates for colorectal cancer (CRC) decreasing • In New Mexico: • Rates for whites decreasing • Rates for Native Americans and Hispanics increasing
Background US CRC screening rate = 57% NM overall CRC screening rate = 50% NM Native Americans = 30% 60% Native Americans have never been screened (BRFSS: 2006)
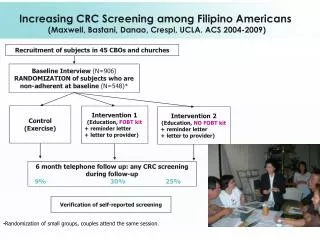
Study Setting: RIOS Net • NM’s primary care, practice-based research network (PBRN) • Voluntary collaboration of 275 clinicians serving medically underserved and culturally diverse communities • Focused on health disparities & translational research
Study Methods • Rigorous qualitative research design • Data collection in 5 IHS (2 Navajo) & 6 CHC (Hispanic) sites • Semi-structured interviews conducted with 1-2 providers, 1 nurse/staff & ~10 patients per site • Surveys administered to patients • Translators provided for patients as needed
Interview & Survey Topics • Interviews focused on: • Cancer causation and prevention • Experiences/impressions of CRC screening tests • Barriers to CRC screening • Surveys focused on: • Health literacy • Exposure to info sources • Prior cancer prevention • Patient-provider communication • Patient decision-making • Recommendations to improve CRC screening • Knowledge about CRC & CRC risk reduction • Access to health care system
Data Analysis • Interview data • Interviews digitally recorded and transcribed • Multidisciplinary team reviewed transcripts • Interviews coded: identified themes explaining barriers and facilitators to CRCS • Survey data • Descriptive statistics with stratification • Hypothesis testing as appropriate (↓ sample size)
Data Collection • Research conducted at Native American sites from June 09 - March 10 • Northern Navajo Medical Center August 17 & 18, 2009 • Tohatchi Medical Center October 26 & 27, 2009 • Navajo sites:
Results: Demographics 5 providers + nurses interviewed 19 Navajo patients interviewed • Language • 15 conducted in English • 4 needed some translation • Gender • 10 (52.6%) female • 9 (47%) male • Age • Mean = 60 years • Range 52-79 years • Education level • 5 (26.3%) had <HS education • 2 (10.6%) had a BA/BS
I. Patient Barriers • Lack of terminology (prevention, cancer, colon) • Cancer not a topic of discussion (taboo) • “Everything’s always hush, hush. You don’t talk about nothing [like that]; it’s just the Navajo way.” –Male patient • Concern that others will know (privacy) • “I would get embarrassed to bring the [FOBT cards] here, I don’t know. I would be embarrassed because they know you, like the staff.” –Female patient
I. Patient Barriers • Personal shame/privacy • “It’s embarrassing to look through your rectum or to get a pap smear, you know, male doctors, I don’t want them to see me.” –Female patient • Fear • “I don't think I want to know if I have something like a cancer. Most people if they find out something is wrong with them, they get more depressed and they think about it, ‘Well, I'm going to die,’ or ‘No, I'm not gonna live long.’” –Male patient • Dietary restrictions: not eating meat (FOBT)
I. Addressing Patient Barriers • Patient education important • Posters around the clinic, take-home educational materials, workshops at the Chapter Houses & Senior Centers • Use of pictures (to address lack of knowledge, literacy & language barriers) • Depersonalize screening to get around taboo • Frame test positively: “making sure you’re healthy” & “taking care of yourself” • Use humor (to address shame & embarrassment)
II. Provider Barriers • Providers don’t bring topic up • Provider turnover • Competing demands • “In a doctor’s visit…you only have a certain amount of time to do certain things. It all depends on how much they can get [in]…a lot of times [nurses] have to explain it.” –Female nurse • Dealing with other illnesses (no time for prevention) • “Preventive health is pretty much always last…because there are very few people who have nothing the matter with them. So there definitely are things that have gone by the wayside.” –Female provider
II. Addressing Provider Barriers • Establishing trust important (intimate topic) • Multiple subsequent description of tests helpful (first the clinician, then nurse in Navajo) • Bundle discussion of CRC into cancer prevention discussions/visits • Schedule CRCS during regular visits (e.g., diabetes) • Be open to blending of Western & traditional approaches
III. System Barriers • Difficult referral system – patients forced to be passive • “I talk to people and get them to agree. Then I fill out this form and send it to the surgery office. And 3 months later they contact the patient. Well, 3 months later, it’s too late.” –Male provider • Capacity • Broken equipment • Patients forced to wait: “I wouldn’t go through the process that my aunt went through. The day of the exam when she went in she said they didn’t get to her ‘til the afternoon.” –Female patient • No screening colonoscopies (no additional insurance)
III. System Barriers • Contract health • Communication capabilities (spotty cell service, no voicemail, distant mailboxes) • Rural setting / transportation: • “A lot of people here on the reservation have a rough time trying to get transportation to get to the provider. So there’s times that they miss appointments or reschedule to where it’ll fit.” –Male patient • Distance to clinic (avg: 27 minutes) • Not having a driver for a colonoscopy • Lack of indoor plumbing for some
III. Addressing System Barriers • Collaborate with auxiliary staff • Nurses/staff can explain tests effectively and bridge language/cultural barriers • Respond to key barriers such as travel and arrange for transportation • Use active CHR program as potential resource for education and transportation
Next Steps • Different levels of engagement/planning (patient-provider-system): • Patient: Development of new educational materials (simple language & pictures); use of storytelling to connect with patients • Provider: Use collaborative approach (provider + nurse + CHR) • System:Tracking and navigation systems need improvement
THANK YOU!!! Christina Getrich chgetrich@salud.unm.edu 505-272-3489