Download
1 / 25
250 likes | 360 Views
CHR Spring Research Update. Norbert Gleicher, MD David H. Barad, MD, MS. Genetically programmed (premature) ovarian aging: the FMR1 gene. Distribution of CGG Triple Repeat Expansions on the FMR1 in the Whole Study Population of Infertile Women in Comparison with a General Population .

E N D
CHR Spring Research Update Norbert Gleicher, MD David H. Barad, MD, MS
Genetically programmed (premature) ovarian aging:the FMR1 gene.
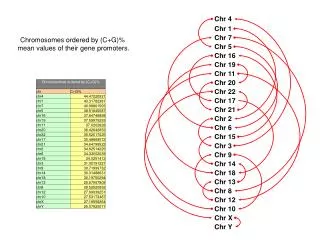
Distribution of CGG Triple Repeat Expansions on the FMR1 in the Whole Study Population of Infertile Women in Comparison with a General Population The figure demonstrates the distributions of CGG triple repeat counts on allele-1 (interrupted line) and allele-2 (solid line) against the shaded background distribution curve reported by Fu et al for a general population. Infertile women demonstrate a mild shift for allele-1and much clearer shift for allele-2 towards higher triple repeats.
Logistic Regressions in Groups A and C The figure represents logistic regressions, demonstrating predicted relative risk (RR) of having AMH of less than 0.8 ng/ml over CGG repeat counts, stratified by age. Blue dots (and blue line) represent women ≥ 38 years of age; Red dots (and green line) represent age < 38 years. The black line reflects women of all ages. RR of diminished ovarian reserve, as reflected by AMH, progressively increases in the presence of CGG counts below and above 30 repeats. For every 5 repeat decrease in CGG count below 30, the relative risk of low AMH increases by 60%. For every 5 repeat increase in CGG repeat count above 30 the relative risk of low AMH is increased by 40%.
Triple CGG Counts by Box and Whisker Plotfor Entire Patient Population
Triple CGG Counts by Box and Whisker Plots for Individual Racial/Ethnic Groups
Normal CGG range: 26-32 Median CGG count: 30
Box and Whisker Plot,Defining Normal AMHLevels and Outliers The figure reflects AMH levels in egg donors and infertility patients based on zygosity in women under age 38 years, when physiological diminution of ovarian reserve due to advancing age affects ovarian function only to a lesser degree. * Denotes one allele in normal count range (26-33) and one allele outside of normal range. ** Denotes both alleles outside of normal range. A reflects egg donors and B infertility patients. The bold horizontal line within each box reflects the median value. AMH values in egg donors did not vary statistically, though they seem to mildly trend upwards from normal to heterozygous and homozygous. Amongst infertility patients results differed significantly between the three patient groups (p=0.032). Specifically, homozygous women demonstrated significantly lower AMH levels than normal patients (p=0.009) and a strong trend towards lower levels in comparison to heterozygous women (p=0.063).
Linear Regression of Association between AMH Levels and Age Based on FMR1 Status The figure represents egg donors and infertility patients at all ages. Normal females at young ages have the highest, and women with homozygous CGG count abnormalities the lowest AMH levels. AMH levels, however, decline in normal women more rapidly than in heterozygous and homozygous patients. At approximately 35 years of age AMH levels in heterozygous women start to exceed those of normal women. AMH levels in homozygous women track those of normal women almost till age 50, when they start exceeding the latter.
AMH Levels in Binned Age Groups Based on FMR1 Status The figure represents egg donors and infertility patients of all ages. Under age 30years AMH levels significantly differ amongst all three patient groups (p=0.009). Specifically, AMH in normal women is significantly higher between normal women and homozygous females (p<0.001) and between heterozygous and homozygous patients (p=0.002). By age 34.99, these statistical differences no longer are present.
Previously ReportedReproductive Benefits of DHEA • Improves egg/embryo numbers • Improves egg/embryo quality • Improves spontaneous pregnancy rates • Improves IVF pregnancy rates • Improves time to conception • Improves cumulative pregnancy rates Carson et al. Hum Reprod 2000 Barad and Gleicher, Hum Reprod 2006 Barad and Gleicher, Fertil Steril 2005 Barad et al, J Assist Reprod Genet 2007
Survival Function for Cumulative Failure to Conceive Stratified by Age 1.2 1.0 .8 Cumulative Failure to Conceive • AGE • >=42 • 38 ->42 • <38 .6 .4 .2 0 2 4 6 8 Months Since Starting DHEA
Premature Ovarian Aging Diminished Ovarian Reserve 0.5 0.4 0.3 0.2 0.1 0.0 0.5 0.4 0.3 0.2 0.1 0.0 Cumulative Pregnancy DHEA DHEA Control Control 0 2 4 6 8 10 0 2 4 6 8 10 Months from Initial Visit Months from Initial Visit Cumulative pregnancy rate based on Cox regression of time from initial visit to clinical pregnancy or censor by DHEA use stratified by ovarian reserve and adjusted for ART treatment, race/ethnicity, age and baseline FSH (HR 3.8; 95% CI 1.2-11.8; p<0.05) Barad et al. J Assist Reprod Genet 2007: 24; 629-634.
Comparison of Miscarriage Rates between DHEA Supplemented Infertility Patients and 2004 National US IVF Outcome Data.
AMH inhibits recruitment and growth La Marca& Volpe: Clinical Endocrinology (2006) 64, 603–610