Download
1 / 19
190 likes | 283 Views
The Association of Iron Deficiency With Swallowing Dysfunction. A presentation of two cases Charles H. Toledo MD FAAP. OVERVIEW .

E N D
The Association of Iron Deficiency With Swallowing Dysfunction A presentation of two cases Charles H. Toledo MD FAAP
OVERVIEW • This presentation describes two patients with oral motor dysfunction of varying severity associated with iron deficiency. It will be obvious from the presentation that this is not a rigorous study; data was gathered retrospectively after the association was made. Caution should be exercised not to draw any firm conclusions regarding this association. Rather this communication is presented in the hopes that it will raise awareness of this possible association and its EASY treatment.
Age 10months • Labs: Hb 11.9 g/dL, Hct 34%, Iron 22.0mcg/dL(40-100), Ferritin 4.0ng/ml(7-140) • Feeding evaluation: Breast milk, honey thick fluids and mashed/pureed foods. • Developmental evaluation: Normal
Age 12 months • Labs: Hb 12.1g/dL, Hct 38%, Iron 8 mcg/dL, Ferritin 40 ng/dL • (The patient had had multiple episodes of otitis media around the time of this evaluation) • Feeding evaluation: Nectar thick fluids and mechanical soft diet • Development: Normal
Age 15 month • Labs None • Feeding evaluation: Cheetos, goldfish, bananas, beans, bread, yogurt, and noodles (cut up) • Development: Normal
Age 18 month • Labs: Iron 86 mcg/dL, Ferritin 10.0 ng/ml, TIBC 374 mcg/dL, Transferrin saturation 22.9% • Feeding evaluation: Completely normal diet including thin liquids. • Development: Normal
Age 2 yrs • Labs: Hb 12.7 g/dL, Hct 40%, Iron 72 mcg/dL , Ferritin 17.7 ng/ml, TIBC 401mcg/dL Transferrin saturation 18% • Feeding evaluation: completely normal diet, including thin liquids. • Development: Normal
Age 24 months • Labs: Hb 12.0 g/dL, Hct 38%, Iron 48 mcg/dL, Ferritin 8.1ng/ml, TIBC 466 mcg/dL, Transferrin 333 mg/dL, Transferrin Saturation 10% • Feeding Evaluation: Immature oral motor skills and oral sensory and tactile sensitivity. Tendency to drool. • Development evaluation: normal
Age 29 months • Labs: Hb 12.7 g/dL, Hct 37%, Iron 19 mcg/dL, Ferritin 24.5 ng/ml, TIBC 365 mcg/dL, Transferrin 261 mg/dL, Transferrin Saturation 5.2% • Feeding evaluation: Improved ability to tolerate more complicated textures and no choking associated with feeding. Marked decrease in drooling. Evaluation still abnormal • Clinical Status: No more breath holding spells.
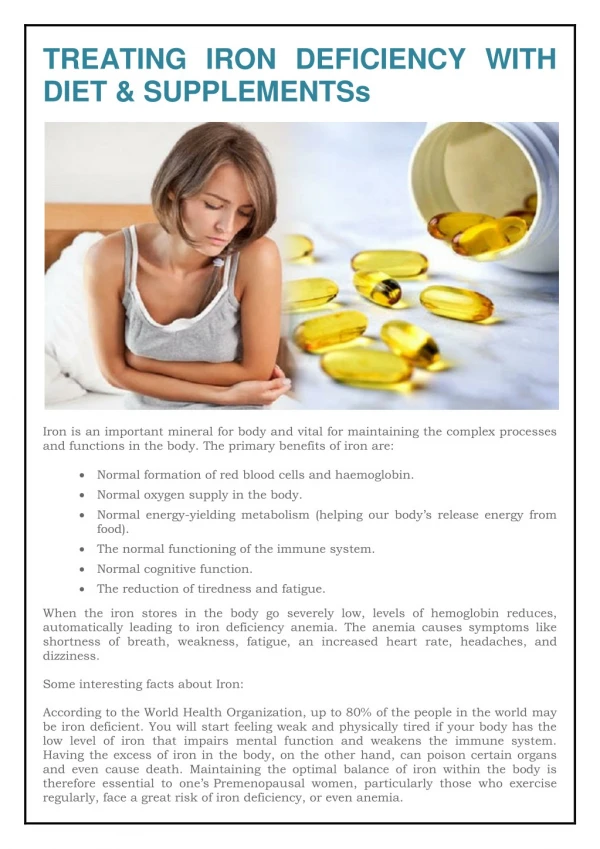
(Insultingly) Brief discussion of iron physiology • Iron is absorbed from our diet by the intestines and most is bound to transferrin, an extracellular transport molecule. • Transferrin bound iron is mainly utilized for processes that are greatly iron dependent (erythropoiesis). Iron stores are reflected by ferritin levels. Deficiency is detrimental for many vital processes (low hemoglobin and decreased oxygen carrying capacity, impact on immunity, growth and development).
The effects of iron deficiency on the developing brain. • Lower cognitive scores that may persist throughout life • Delay in motor development • Altered social and emotional development
Iron deficiency and breath holding spells • Cyanotic breath holding spells have been associated with iron deficiency. Poets et al (Acta Paediatrica, 1992). • In this report 41 infants with a history of life threatening breath holding spells are described: 34 of which had Hb below mean, and 7 had Hb at or above mean.
Iron deficiency and breath holding spells Colina et al (J. Peds, 1994) describe two children with severe breath holding spells and anemia. BHS resolved with iron therapy.
Iron deficiency and swallowing dysfunction • Iron Deficiency has been associated with postcricoid dysphagia, upper esophageal webs and glossitis in a condition described as Plummer-Vincent Syndrome. • This is now a rare condition due to iron supplementation of food products. • Although mainly described in elderly women, there have been case reports in children. (Mansell et el, J. Laryngol Otol ,1999)
Iron deficiency and swallowing dysfunction • Experimental Iron Deficiency induced in rabbits creates changes preferentially in the muscles utilized in swallowing. • Iron deficiency also occurs in these muscles. • These changes were not noted in neck or femoral muscles. (Tsutsumi, S 1993)
Conclusion • There may be an association between swallowing dysfunction and iron deficiency in infants and children. • Breath holding spells may be involved in this process. • Hemoglobin and hematocrit levels may not be reflective of iron status in these infants. • One may consider evaluating the iron status of infants and children with swallowing dysfunction, especially if associated with breath holding spells