Download
1 / 50
500 likes | 650 Views
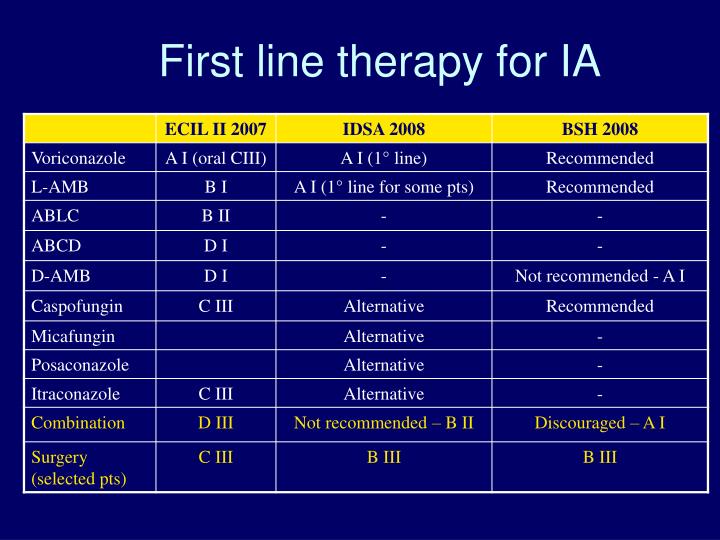
First line therapy for IA. Salvage therapy. Pivotal factors associated with evaluation of outcome in IA. Reaching the right blood levels with voriconazole Disease certainty Micro-confirmed vs non micro-confirmed Underlying condition Status of underlying disease

E N D
Pivotal factors associated with evaluation of outcome in IA • Reaching the right blood levels with voriconazole • Disease certainty • Micro-confirmed vs non micro-confirmed • Underlying condition • Status of underlying disease • Transplant vs non transplant • Type of transplant • Neutropenia • Outcome definition
Pharmacokinetics of Voriconazole Influence of CYP2C19 genotype FDA - Briefing document for Voriconazole - Pfizer, October 2001 courtesy of Dr. N. Wood, Pfizer Central Research
Voriconazole: variability of blood concentrations Pascual A et al. CID 2008; 46:201-211
Voriconazole trough blood levels and clinical response to antifungal therapy Pascual A et al. CID 2008; 46:201-211
Voriconazole trough blood levels and safety of antifungal therapy Pascual A et al. CID 2008; 46:201-211
Pivotal factors associated with evaluation of outcome in IA • Reaching the right blood levels with voriconazole • Disease certainty • Micro-confirmed vs non micro-confirmed • Underlying condition • Status of underlying disease • Transplant vs non transplant • Type of transplant • Neutropenia • Outcome definition
Fungalinfection: levelofcertainty Proven Probable Possible
Probableinvasive fungal infection Host factors One major or 2 minor clinical criteria One micro criterion + +
Modified EORTC_MSG criteria used in many clinical trials Host factors Clinical criteria (halo sign) One micro criterion + +
HR (95% CI) P Proven IA 2.2 (1.5-3.2) <.0001
Reference category HR (95% CI) P Degree of certainty of IA diagnosis Possible vs.Proven or probable 0.5 (0.3-0.9) .010
Drug performance in patients with “true” probable/proven IA • Denning, vorico phase II • Response overall 54% • Response in proven/probable 38% • Herbrecht, vorico phase III • Response overall 53% • Response proven/probable 46% • Ambiload, 3 mg/Kg arm • Response overall 50% • Response proven/probable 39% • Caspofungin • Only proven/probable (both AL and HSCT) 35% EXTRAPOLATED FROM AVAILABLE PUBLICATIONS
Pivotal factors associated with evaluation of outcome in IA • Reaching the right blood levels with voriconazole • Disease certainty • Micro-confirmed vs non micro-confirmed • Underlying condition • Status of underlying disease • Transplant vs non transplant • Type of transplant • Neutropenia • Outcome definition
Upton et al CID 2007
Week 12 successful response rate (%) Vori Ampho B 53 32 55 34 43 13 32 13 63 38 50 32 51 32 54 32 45 20 60 37 50 28 Favors vori Favors AmB Overall (MITT) Pulmonary only Extra pulmonary Allogeneic HSCT Other hemat. dis. Other Neutropenic Non-neutropenic Definite IA Probable IA Overall (ITT) -20 0 20 40 60 Difference in proportions (%) and 95% CI
BMT 2009 • In our study, a relapsing underlying disease • was strongly associated with the risk of developing • invasive aspergillosis and was also associated with the • risk of dying from aspergillosis (OR=3.8)
Multicenter, open, phase II study to estimate the activity and safety of caspofungin as first-line therapy of probable and proven invasive aspergillosis in:-patients with hematological malignances or recipients of autologous HSCT-recipients of allogeneic HSCT Viscoli C, Herbrecht R, Akan H, Baila L, Doyen C, Gallamini A, Giagounidis A, Marchetti O, Martino R, Meert L, Paesmans M, Shivaprakash M, Ullmann AJ and Maertens J for the Infectious Disease Group of the EORTC 8
The EORTC studies of caspofungin in IA • Open label, phase II, non comparative studies in: • Hematological patients undergoing standard chemotherapy or autologous HSCT • Hematological patients undergoing allogeneic HSCT
Main methodological characteristics • Only patients with proven/probable IA (i.e. only cases supported or proven by positive microbiology or GM antigen detection test). • Sample size calculation based on results of the only available study, at that time, although designed differently, i.e. the voriconazole vs. AmB deaxy study (52% for standard chemo, 32% for allaHSCT) • Very sick patients not excluded a priori • Evaluation End of Treatment (EOT) • Patients with less than 50% reduction in the sum of the areas at CT scan considered as stable disease (i.e. failure) at EOT
Schema of the study HM or auto/allo HSCT Signs, symptoms and/or laboratory/radiological data suggestive of probable/proven/possible IA Proven/probable Possible Registration/start study treatment Upgraded to probable/proven IA within 7 days from registration, based on tests performed prior to or within 48 hrs after registration Continue study treatment Yes No Stop study treatment (evaluable for safety) End of study treatment (min 14 days – max 84 days) SUCCESS FAILURE Shifting to oral drugs allowed for maintenance or secondary prophylaxis Further treatment at the discretion of the investigator 12
Efficacy Response at EOT by Specific Outcome – MITT Analysis
Factor associated with survival at multivariate analysis (57/61 pts) Only hematological patients 32
Survival at 12 weeks in the caspofungin, voriconazole and liposomal-AmB trials Vorico D-AmB L-AmB3 L-AmB10 Caspo Overall In pts with non progressing Cancer In pts with progressing cancer 71 58 72 59 54 ? ? 81 93 ? ? 54 40 Numbers are percentages
Week 12 successful response rate (%) Vori Ampho B 53 32 55 34 43 13 32 13 63 38 50 32 51 32 54 32 45 20 60 37 50 28 Favors vori Favors AmB Overall (MITT) Pulmonary only Extra pulmonary Allogeneic HSCT Other hemat. dis. Other Neutropenic Non-neutropenic Definite IA Probable IA Overall (ITT) -20 0 20 40 60 Difference in proportions (%) and 95% CI
Caspo study EORTC All differences are not statistically significant
Pivotal factors associated with evaluation of outcome in IA • Reaching the right blood levels with voriconazole • Disease certainty • Micro-confirmed vs non micro-confirmed • Underlying condition • Status of underlying disease • Transplant vs non transplant • Type of transplant • Neutropenia • Outcome definition
Outcome Definitions(Standard Response Criteria) Complete Response Resolution of all attributable clinical signs and symptoms No new clinical signs or radiological abnormalities compatible with IA Disappearance of all radiological lesions attributable to aspergillosis. Partial Response Major improvement of fever and attributable clinical signs and symptoms No new clinical signs or radiological abnormalities compatible with IA At least 50% decrease in the sum of the area of the attributable measurable lesions; Progression Worsening of clinical signs and symptoms New clinical signs or radiological abnormalities compatible with IA Increase in the sum of the area of the attributable measurable lesions Stable Disease Criteria for complete or partial remission or progression are not met
Correlation between EOT response and change in size of the radiological lesions (available in 45/61 pts) Only hematological patients 29
CR/PR (N = 20) SD (N = 9) PD (N = 31) Difference in size of the lesions N 19 8 30 Median (95% CI*) Reduction of 75% (65%-82%) Reduction of 36% Increase of 103% (69% - 421%) Fever Improvement 55% (11/20) 78% (7/9) 32% (10/31) Stabilization 40% (8/20) 22% (2/9) 61% (19/31) Deteroriation 5% (1/20) - - 6% (2/31) Galactomannan Improvement 64% (9/14) 100% (6/6) 42% (11/26) Stabilization 36% (5/14) - - 50% (13/26) Deteroriation - - - - 8% (2/26) Sputum production Improvement 30% (6/20) 11% (1/9) 19% (6/31) Stabilization 65% (13/20) 89% (8/9) 71% (22/31) Deteroriation 5% (1/20) - - 10% (3/31) Cough Improvement 45% (9/20) 67% (6/9) 33% (10/30) Stabilization 45% (9/20) 22% (2/9) 47% (14/30) Deteroriation 10% (2/20) 11% (1/9) 20% (6/30) Dyspnea Improvement 40% (8/20) 33% (3/9) 6% (2/31) Stabilization 55% (11/20) 44% (4/9) 35% (11/31) Deteroriation 5% (1/20) 22% (2/9) 58% (18/31) Chest Pain Improvement 30% (6/20) 56% (5/9) 24% (7/29) Stabilization 70% (14/20) 44% (4/9) 76% (22/29) Deteroriation - - - - - - There was no clinical difference between patients with partial remission and stable disease. The only difference was in the degree of reduction in the size of the lesion
Conclusion • Voriconazole blood levels should probably be monitored • Results of therapy of IA may vary substantially based upon: • Disease certainty • Severity of underlying conditions • HSCT vs non HSCT (???) • Role of neutropenia not clear • A stable disease might be considered as success in very sick patients
Infections in compromised patients are unique because we treat an infection in a patient with another disease. The backgroud noise of the other disease is crucial in evaluating the results of the antinfective therapy
HR (95% CI) P Proven IA 2.7 (2.0-3.7) <.0001
Including possible HR (95% CI) P Degree of certainty of IA diagnosis Possible vs Proven or probable 0.5 (0.3-0.8) .001 Nivoix et al, CID 2008
Upton et al CID 2007
Response to treatment with stable disease as failure or success with vorico, L.Amb, caspo(Numbers are percentages) • Vorico (NEJM 2002) 52vs58 • L-AmB 3 (CID 2007) 50vs57 • Caspo (TIMM 2007, ICAAC 2008) 35vs47 Just an exercise. I know that different studies cannot be compared
Outcomes by neutropenia P value for response EOT by history of neutropenia= 0.04 All other p values are not statistically significant