Download
1 / 40
400 likes | 528 Views
A 58 yo Man with Dizziness and Sweating. Susan Poe, MD Primary Care Conference 9/13/06. Case.

E N D
A 58 yo Man with Dizziness and Sweating Susan Poe, MD Primary Care Conference 9/13/06
Case • 58 yo male with hx of IDDM and chronic migraine headaches presents with complaints of tremor and dizziness. c/o gradual onset of shakiness and difficulty with gait. Described a tremor at rest such as resting his hand on the gear shift. Intermittent dizziness was described as a lighted headed sensation and as an unsteady gait. Has to hold on to the wall to prevent falling over. Wife described jerking legs at night. Also notes he seems jerky in general such as being easily startled.
Case cont. Denies change in vision, urinary or bowel control. No numbness or weakness. Denies vertigo, nausea, diarrhea. Blood sugars have been up and down as usual. Migraine headaches are unchanged.
PMH Chronic MHA-on pain contract IDDM since childhood Gastroparesis, periph neuropathy No retinopathy or nephropathy Fibromyalgia Restless legs Hyperlipidemia Depression Remote hx IV drug abuse
Asa Cyclobenzaprine 10 tid Benadryl 25 bid Eletriptan 20 mg qd Lexapro 40 mg qd Hydromorphone 2mg IM 2x/wk Hydroxyzine 50 mg im 2x/wk Insulin per pump Metoclopramide 10 qid Protonix 40 mg qd Oxytryptan powder Zocor 20 mg qd Verapamil 120 mg qd Albuterol inhaler prn L-dopa recently d/ced Meds
PE Alert and oriented , NAD BP 98/64, P 84 HEENT- pupils sl dilated but responsive Chest clear to A & P CV RRR no m,g,r No carotid bruits Abd- benign
PE cont Neuro exam: Alert and oriented Romberg neg, heel to toe walk wobbly No resting tremor noted Finger to nose and heel to shin sluggish but intact Reflexes absent (chronic) Positive cogwheeling
Impression Possible parkinsonian symptoms Recommend d/c metoclopramide
F/up Urgent Care visit Syncope after arising from sofa Fractured a rib Since d/cing metoclopramide tremor is a little better but other symptoms persist. Reviewed his meds and decided to make some changes.
Objective Increase recognition of a common usually mild but potentially serious toxicity Understand how to differentiate it from other similar toxicities Appreciate the pathophysiology so that one might be able to prevent it Understand management principles
Financial disclosure No financial incentives for this talk
Serotonin syndrome Clinical triad: MS change, autonomic hyperactivity, neuromusc hyperactivity Clinical spectrum of symptoms due to toxicity, usually mild but potentially life threatening Increased stimulation of serotonin receptors
Why the concern • Mild cases easily overlooked which could lead to severe symptoms if new drug introduced or change in dose • Almost all fatal and most severe cases due to drug combinations. • 1980’s Libby Zion case: meperidene plus MAOI
All age groups Increasing incidence parallels increasing use of serotonergic agents SS occurs in 14-16% of SSRI overdoses Epidemiology
Protean manifestations Strict application of diagnostic criteria can rule out mild or sub acute cases Physician unawareness 85% Striking number of drugs and drug combinations are associated with SS. Barriers to diagnosis
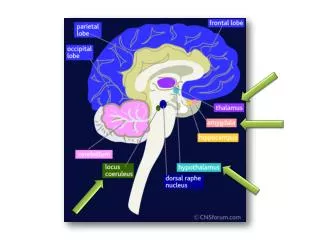
L-tryptophan converted to serotonin in presynaptic neuron Incorporated into vesicles Axonal stimulation releases serotonin Binds to postsynaptic receptor Reuptake into presynaptic neuron Metabolized by monoamine oxidase A Serotonin pharmacology
Multiple Receptors Implicated 5-HT1A 5-HT2A Probably others indirectly
Rapid onset and resolution Usually present within 24 hrs of new drug or change in dose 60% present within 6 hours Respond within 24 hours usually Exception: sub acute cases, drugs with long half lives
Clinical Triad Mental Status Changes Autonomic Manifestations Muscular hyperactivity
Mental Status Changes Anxiety, restlessness, startle easily Agitated delirium, disorientation
Autonomic Hyperactivity Diaphoresis very common Dry mucous membranes Mydriasis, shivering Tachycardia, htn Vomiting, diarrhea, hyperactive BS’s Hyperthermia in severe cases
Neuromuscular Hyperactivity • Hyperreflexia • Clonus, myoclonus, B babinskis • Ocular clonus • Tremor, neuromuscular rigidity • Most pronounced in the LE’s
Agitated delirium Severe htn, tachy Muscular rigidity, hypertonicity Hyperthermia due to muscle hyperactivity Rhabdomyolysis, seizures, renal failure, DIC Severe case
Diagnosis Clinical Does not correlate with drug levels Differential diagnosis Hunter criteria
Differential diagnosis Neuroleptic malignant syndrome (dopamine antagonist) Develops and resolves over days to wks Neuromuscular sluggishness, bradyreflexia Anticholinergic toxicity Mydriasis, dry mucous membranes Urinary retention, decreased bs’s Normal muscle tone and reflexes Malignant hyperthermia Rigor mortis like rigidity Develops within minutes Halogenated anesthetics, depolarizing relaxants
Hunter Criteria: 84% sens, 97% specDrug plus one of the following: Spontaneous clonus Inducible clonus + agitation or diaphoresis Ocular clonus + agitation or diaphoresis Tremor and hyperreflexia Hypertonia Temp > 38 deg + ocular or inducible clonus
Drugs • Single dose of SSRI can cause syndrome • MAOI’s associated with severe or fatal cases if combined with SSRI, meperidene, dextromethorphan, MDMA • Drugs that affect cytochrome P450 system • Prolonged effect with long ½ life. Adding serotonergic drug within 5 wks of d/cing fluoxetine • Drug level doesn’t correlate with toxicity
Treatment Remove precipitating drug Benzodiazepines for agitation No physical restraints Chemical paralysis if hyperthermic Cyproheptadine, 5-HT2A antagonist Olanzapine, chlorpromazine
Treatment cont. Hypotension: low dose direct acting sympathomimetic amines ie norepi, epi Avoid dopamine –prolonged htn Htn, tachy- short acting agents ie nipride, esmolol, avoid propranolol (long acting 5HT1A antagonist) Bromocriptine, rx for NMS, can exacerbate
Treatment cont. If not sure of diagnosis, supportive care: Benzodiazepines IV fluids Chemical sedation Short acting agents for htn and hypotension
This patient’s drugs: Cyclobenzaprine: anticholinergic Benadryl: antihistamine, inhibits P450 Eletriptan: serotonin receptor agonist Lexapro: SSRI Hydroxyzine: antihistamine Metoclopramide: dopamine antagonist Verapamil: inhibits P450 Oxytryptan: serotonin precursor
f/up Discontinued metoclopramide – no significant response Discontinued verapamil – symptoms improved Final diagnosis: polypharmacy with serotonin toxicity likely exacerbated by adding p 450 inhibitor.
Summary SS is a clinical spectrum of toxicity Rapid onset and rapid resolution with medication change Triad of MS change, autonomic and neuromuscular hyperactivity Distinguishing features: clonus, agitation, diaphoresis, tremor and hypereflexia
Summary cont. Diagnosis requires clinical suspicion esp. in mild cases Important to recognize mild case if adding additional agent that affects serotonin neurotransmission Treatment is supportive Antidote cyproheptadine Prevention requires awareness of multiple drugs affecting serotonin stimulation
Bibliography Boyer e al. The serotonin syndrome. NEJM 2005; 352:1112. Kent et al. Serotonin syndrome. UpToDate 2006. Ganesky. Selective serotonin reuptake inhibitor intoxication. UpToDate. 2006. Dunkley et al. The Hunter Serotonin Toxicity Criteria. QJM 2003; 96: 635. Isbister e al. The Pathophysiology of Serotonin Toxicity in Animals and Humans. Clinical Neuropharmacology. 2005. 28 (5):205.