Download
1 / 26
260 likes | 361 Views
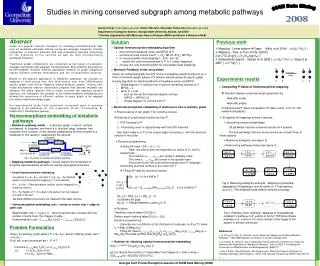
Pathways and TEAMcare Studies. Wayne Katon, MD 1 Mike VonKorff, ScD 2 Elizabeth Lin, MD, MPH 2 Paul Ciechanowski, MD, MPH 1 Evette Ludman, PhD 2 Carolyn Rutter, PhD 2 Bessie Young, MD, MPH 1 Do Peterson, MS 2 David McCulloch, MD 2. 1 University of Washington School of Medicine

E N D
Pathways and TEAMcare Studies Wayne Katon, MD1 Mike VonKorff, ScD2 Elizabeth Lin, MD, MPH2 Paul Ciechanowski, MD, MPH1 Evette Ludman, PhD2 Carolyn Rutter, PhD2 Bessie Young, MD, MPH1 Do Peterson, MS2 David McCulloch, MD2 1University of Washington School of Medicine 2Group Health Research Institute NIMH Grants MH 41739 and MH 01643 (Dr. Katon)
Health Services Models • TEAMcare approaches have been shown to improve quality of care and outcomes of patients with depression, diabetes, asthma and CHF • The most complex and medical costly patients often have multiple comorbidities including at least one mental health diagnosis
Medicare Patients • Depression, diabetes and heart disease are among the most common illnesses in aging populations but fewer than 4% of Medicare beneficiaries with any of these three illnesses have no other chronic medical conditions • 80% of those with CHF, 71% with depression and 56% with diabetes have 4 or more chronic conditions • Partnership for Solutions 2001
161,697 Patients with Diabetes were Examined to Estimate Rates and Reasons for Poor Disease Control (HbA1c, SBP, LDLs) • 20% to 23% poor adherence • Among those with adequate adherence, 30% to 47% had no evidence of treatment intensification • Poor adherence and lack of treatment intensification were found in 53% to 68% of patients with poor disease control Schmittdiel J, et al. 2008
Challenge: Development of Health Services Models for “Natural” Clusters of Illness • Definition: Illnesses with high prevalence, high comorbidity and bidirectional adverse interactions • Examples: • Diabetes, CAD, depression • Depression, chronic pain, substance abuse
New NIMH-Funded Study: TEAMcare Inclusion Criteria • Evidence via automated date (ICD-9) of having diabetes and/or coronary artery disease (CAD) • Evidence of poor disease control (HbA1c >8.5, blood pressure >140/90, LDL >130) • PHQ-9 >10
Recruitment • 14 GH clinics (e.g. Olympia, Everett, Silverdale, and BVU) • 150 primary care physicians signed consent • 9,838 PHQ-2 screeners mailed • 214 Patients randomized • 106 Intervention (106) • 108 Control
TEAMcare Intervention Goals • Improve depression care: behavioral activation and antidepressants • Improve medical disease control: HbA1c, HTN, LDL • Improve self-care (diet, exercise, cessation of smoking, glucose checks)
Core Elements • Nurse Care Management • Identify Goals – specific, measurable (BP, HbA1c, PHQ-9, # steps) • Monitor Progress of Targets – systematic, pro-active • Treat-to-Target – relentless adjustment, INDIVIDUALIZED • Support Self-Care – adherence to medication adjustments • Regular Clinical Review – supervised case reviews, Tx recommendations
TEAMcare Interventionists • 3 diabetes nurse educators • Caseload supervision • Depression: 2 psychiatrists • Diabetes and CAD: nephrologist, family doctor • E-Mail to diabetologist for complex cases
Nurse Training • Motivational interviewing • Problem solving • Behavioral activation • Antidepressants • TREAT-to-TARGET: blood glucose, HTN, LDLS
Improving Adherence • Patient self-care materials: book and video on depression, patient manual (Tools for Managing Your Chronic Disease) • Nurse support/education/motivational interviewing • Medisets • Simplifying medication regimen • $4 generics to avoid $10 co-pays
Self-Care Enhancements • Glucometers: Group Health provides • Home blood pressure monitors • Pedometers to increase exercise • Medisets to improve adherence
Phases of Treatment • Intervene on depression initially • Behavioral activation • Antidepressant medication
Medical Disease Control • Is patient adhering to medication regimen? • If adhering and in poor control, is patient on optimal dosage? • If maximum dosage has been reached should a new medication be tried instead or augmentation of initial medication? • Team recommendations of medication changes are reviewed with primary care physician for approval
TREAT-to-TARGET Guidelines • Nurses ask for physician approval for gradually increasing insulin or blood pressure medications based on these guidelines
Behavioral Goals • Behavioral activation/exercise • Dietary changes • Checking blood glucose/altering insulin • Cessation of smoking
Satisfaction with Care of Depression p < .001 p < .001 months
Satisfaction with Care of Diabetes and/or CHD p < .001 p < .001 months
Conclusions • Economies of scale: New health services interventions are needed for patients with multiple comorbidities (one of which is a psychiatric disorder). • The TEAMcare model is a promising approach to improving depression and medical disease control.