Download
1 / 62
1.14k likes | 3.46k Views
PROSTATITIS. Presented by Dr.Bandar Al Hubaishy KAUH. Epidemiology. Prostatitis is the most common urologic diagnosis in males<50 years and the The third most common diagnosis in men>50 years

E N D
PROSTATITIS Presented by Dr.Bandar Al Hubaishy KAUH
Epidemiology • Prostatitis is the most common urologic diagnosis in males<50 years and the • The third most common diagnosis in men>50 years • Of 600 men diagnosed with prostatitis, 5% had bacterial prostatitis, 64% had nonbacterial prostatitis, and 31% had pelvic-perineal pain syndrome
Category I: Acute Bacterial Prostatitis • It is caused by bacterial infection of the prostate gland. • It is much less common than chronic prostatitis but is easier to identify
Pathophysiology • Microbiologic causes • Risk Factor
Microbiogic Causes • Gram-negative members of the Enterobacteriaceae family. • They include Escherichia coli, Proteus mirabilis, Klebsiellaspecies, Enterobacter species, Pseudomonas aeruginosa, and Serratia species. • E coli is responsible for 65% – 80% of the cases • Pseudomonas aeruginosa, and Serratia species are responsible for 10% - 15%
Microbiogic Causes • Obligate anaerobic bacteria and gram-positive bacteria other than enterococci rarely cause acute bacterial prostatitis. • Enterococci account for 5-10% of documented prostate infections. • Staphylococcus aureus infection due to prolonged catheterization may occur in the hospital.
Microbiogic Causes • Other occasional causative organisms include Neisseria gonorrhea,Mycobacterium tuberculosis,Salmonella species, Clostridium species, and parasitic or mycotic organisms. N gonorrhea should be suspected in sexually active men younger than 35 years.
Risk Factors • Intraprostatic urinary reflux
Risk Factor • Ascending urethral infection • sexual intercourse • instrumentation • prolonged catheterization • Direct invasion or lymphogenous spread from the rectum • Direct hematogenous infection • Unprotected anal intercourse • Acute epididymitis • Altered prostatic secretions • Phymosis and redundant skin
Clinical presentation • Systemic symptoms: fever,chilis, malaise, arthalgia, vomiting, septicemia and hypotension • Irritative symptoms: dysuria, frequency, urgency • Obstructive symptoms: hesitancy, poor interrupted stream, strangury, and even acute urinary retention are common. • Perineal and suprapubic pain
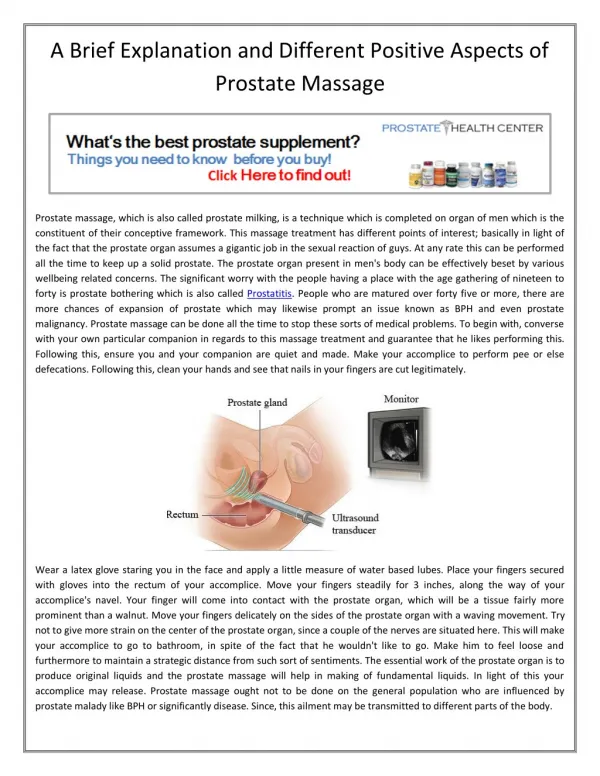
Physical Examination • Vitals • Abdomen Ex • DRE: enlarged, tender, firm prostate gland Note:avoid vigorous prostatic massage in a patient with suspected acute bacterial prostatitis to prevent bacteremia and sepsis.
Work up • Complete blood count: leukocytosis • Urine analysis: It shows large number of WBC • Urodynamics: Helps to avoid misdiagnosis of prostatitis
Work up • Serumprostate-specific antigen: PSA has little to no clinical value. If the PSA level is obtained and is found to be elevated the study should be repeated 30-60 days after adequate treatment.
Work up • Imaging Studies : CT scanning of the pelvis ortransrectal ultrasonography • Indications: 1-Laboratory analysis findings are equivocal 2- No improvement is observed following medical therapy. 3- Ruling out complications of prostatitis (eg, prostatic abscess)
Work up • Prostate biopsy: It is contraindicated in cases of suspected acute bacterial prostatitis • Complications: 1-Seeding the bacterial infection in adjacent organs. 2-Sepsis.
Managemet • Medical treatment • Surgical Treatment
Medical treatment • Supportive therapy: Antipyretics, analgesics, stool softeners, bed rest, and increased fluid intake provide • Urinary retention: A Foley catheter can be inserted gently for drainage if severe obstruction is suspected. A punch suprapubic tube can be used if a catheter cannot be passed easily or is not tolerated by the patient. The catheter can be removed 24-36 hours later.
Medical treatment • Antibiotic therapy The initial therapy must be directed to Gram-ve microorganism. Useful agents include fluoroquinolones, trimethoprim-sulfamethoxazole, and ampicillin with gentamicin.
Medical treatment • Intravenous therapy, use trimethoprim-sulfamethoxazole (Bactrim), 8-10 mg/kg/d (based on the trimethoprim component) in 2-4 intravenous doses bid, tid, or qid until the culture and sensitivity results are known. An alternate regimen is gentamicin with ampicillin 3-5 mg/kg/d IV (gentamicin dose divided tid and 2 g ampicillin divided qid).
Medical treatment • If the initial clinical response to therapy is satisfactory, treatment is continued orally for 30 days to prevent sequelae such as chronic bacterialprostatitis and prostatic abscess formation.
Medical treatment • For oral therapy, Use trimethoprim-sulfamethoxazole (Bactrim), 160 mg of trimethoprim and 800 mg of sulfamethoxazole, PO bid for 30 days. Use levofloxacin (Levaquin) 500 mg PO bid; ciprofloxacin, 500 mg PO bid; norfloxacin, 400 mg PO bid; ofloxacin, 400 mg PO bid; or enoxacin, 400 mg PO bid for 30 days when clinical response is favorable.
Medical treatment • Alpha-blocker therapy : • It improve outflow obstruction and diminish intraprostatic urinary reflux • Terazosin 5 mg/d PO for 4-52 wk, Tamsulosin (Flomax), alfuzosin (UroXatral) and doxazosin (Cardura) are acceptable alternatives
Complication of acute prostatitis • Prostatic Abscess • Progression to chronic prostatitis, septicemia, • Pyelonephritis, and • Epididymitis.
Surgical Treatment Indication: Prostatic Abscess
Prostatic abscess • Prostatic abscess is an uncommon but well-described. • Coliform bacteria, especially E coli, cause more than 70% of prostatic abscesses • Risk Factors: Immunocompromised DM Urethral instrumentation. Prolonged indwelling urethral catheters. Patients on maintenance dialysis.
Management • Clindamycin intravenously at 600-900 mg q8h or orally at 150-450 mg q8h is a good choice. However, medical management is often unsuccessful. • Transrectal or perineal aspiration of the abscess if symptoms do not improve after 1 week of medical therapy. • Transurethral resection of the prostate and drainage of the abscess. Recurrent abscesses are rare. The abscess should be allowed to drain and should be monitored closely if a spontaneous rupture occurs into the urethra.
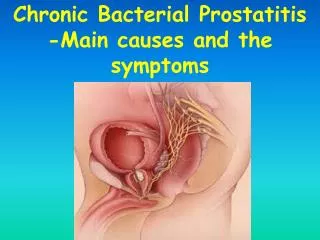
Category II: Chronic Bacterial Prostatitis • 35-55% of men have prostatitis symptoms. • Recent studies show that prostatitis has the same effect on a patient's mental health as does diabetes mellitus and congestive heart failure. • Recent studies using the US National Institutes of Health-Chronic Prostatitis Symptom Index (NIH-CPSI) found that the prevalence of prostatitis symptoms was 10% in a population of men aged 20-74 years.
Clinical Presentation • Genitourinary pain it occurs in the perineal area, penile tip, testicles, rectum, lower abdomen, and back. • Patients can also have irritative or obstructive urologic symptoms • Other symptoms include a clear-to-milky urethral discharge, ejaculatory pain, hematospermia, and sexual dysfunction.
Physical Examination • Physical examination findings are often nonspecific • The classic presentation : an enlarged, soft, or, boggy gland that is moderately-to-severely tender upon palpation. • In some cases, an examiner is able to palpate prostatic stones..
Pathophysiology • Predisposing factors: Acute bacterial prostatitis Prostatic calculi Uretheral stricture and refluxing urine
Pathology • Escherichia coli • Klebsiella pneumoniae • Pseudomonas aeruginosa • Proteusspecies • Staphylococcusspecies • Enterococcusspecies • Trichomonasspecies • Candidaspecies • C trachomatis • U urealyticum • M hominis
Work up • The 2 glass test Positive urine culture findings after a prostatic massage Criteria for the diagnosis: 1- WBCs in an EPS is more than 10 WBCs/hpf (40X objective) or an observation of clumping WBCs with the presence of oval fat bodies 2- a positive EPS culture finding
Work up • Imaging Studies: Transrectal Ultrasound or CT pelvis It is useful for detecting prostaric calculi • Prostate biopsy:
Work up • If the patient has frequent recurrences of chronic prostatitis, other tests may help exclude an anatomic obstruction due to: 1- prostatic hyperplasia, 2- urinary stricture disease, 3- bladder neck dysfunction. • Retrograde urethrography, uroflowmetry, and postvoid residual testing and cystoscopy.
Management • Antimicrobial therapy: The Ideal antibiotics must have: 1- Higher dissociation constant to allow diffusion of their un-ionized components into the prostate. 2-The antibiotic must be basic, it can readily concentrate much in the gland
Management • The best antibiotic choices include 1-trimethoprim-sulfamethoxazole (TMP-SMZ) at 80-400 mg given twice a day 2-fluoroquinolone antibiotics (eg, ciprofloxacin at 500 mg or ofloxacin at 400 mg) twice a day 3-gatifloxacin/moxifloxacin at 400 mg daily. NOTE :TMP-SMZ yields a 33-50% cure rate with a 4- to 6-week course of treatment. Fluoroquinolones yield a similar cure rate with a 4-week course.
Management • If oral antibiotic therapy fails, use other antibiotics. • These may include carbenicillin or doxycycline or injections of gentamicin, either parenterally or directly into the prostate.
Management • Persistent infections, especially those who have symptom improvement while on antibiotics but quickly have a recurrence after finishing a course of antibiotics, may benefit from suppressive therapy with low daily doses of antibiotics. • Good choices are tetracycline, nitrofurantoin,nalidixicacid, cephalexin, or trimethoprim.
Management • Nonsteroidal anti-inflammatory drugs and alpha-blockers . • Surgical Treatment TURP or TUVP are not indicated except in certain condition when a patient has recurrent episodes of chronic prostatitis and improves with antibiotics
Category III: Chronic Pelvic Pain Syndrome • There is no difference between Category IIIA and Category IIIB • It is the most common category of prostatitis • It affects the quality of life
Pathophysiology • The etiology (or etiologies) of CPPS remains unknown • Special signaling molecules called cytokines, which are produced by WBCs (and by other cells), may play a role. • Genetic factors • Autoimmunity,
Pathophysiology • Testosterone • Abnormal functioning of the nervous system • Psychological stress and depression
Clinical presentation • The predominant is pain, which was most commonly localized to the perineum, suprapubic area, and penis but can also occur in the testes, groin, or low back. • Pain during or after ejaculation is one of the most prominent, important, and bothersome feature in many patients .
Clinical presentation • Irritative and obstructive voiding symptoms including urgency, frequency, hesitancy, and poor interrupted flow are associated with this syndrome in many patients. • Erectile dysfunction and sexual disturbances .
Clinical presentation • The syndrome becomes chronic after 3 months' duration. • The symptoms tend to wax and wane over time; • The impact of this condition on health status is significant.
Chronic Prostatitis Symptoms Index • Pain symptoms (4 questions): Q1-In the past week, have you experienced any pain (1) between your rectum and testicles, (2) in the testicles, (3) in the tip of the penis, or (4) below your waist? Q2-In the past week, have you experienced pain or burning upon urination or pain or discomfort during or after sexual intercourse?
Chronic Prostatitis Symptoms Index Q3 -How often have you had pain in any of the above areas over the last week? Q4 -Over the last week, which number (1-10) best describes your average pain or discomfort on the days that you had it?