Download
1 / 37
400 likes | 894 Views
Update on Prostatitis and Treatments. BAUN Benign Study Day 14/03/2012 Mr Richard Cetti Specialist Registrar Urology, QA Portsmouth. Prostatitis an Important Problem!. Prevalence 2.2-13.8% Quality of life Economic Costs. Prostatitis an Important Problem!.

E N D
Update on Prostatitis and Treatments BAUN Benign Study Day 14/03/2012 Mr Richard Cetti Specialist Registrar Urology, QA Portsmouth
Prostatitis an Important Problem! • Prevalence 2.2-13.8% • Quality of life • Economic Costs
Prostatitis an Important Problem! • ‘Pain management is a necessity in the work of each physician.’ F. Sauerbruch, 1936
Introduction • Pain • Classification/Terminology • Presentation • Investigation • Treatment- historical, contemporary and the evidence • The Future
Pain-an unpleasant sensory and emotional experience Hypogastric Nerve Pelvic Nerves Pudendal Nerve Convergence Projection Theory (Ruch) Skin Viscus
Chronic Pain • Combination of: • Neuroplasticity • Central processing altered • Trophic changes in subcutaneous tissue and muscle • All site normal sensations become painful (allodynia). • At site painful stimuli become more painful (hyperalgesia). • Zone affected adjacent tissue (secondary hyperalgesia).
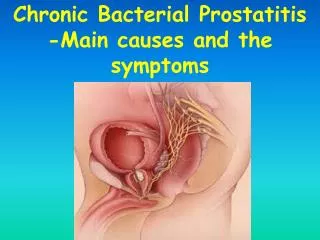
Aetiology of Chronic Prostatitis • Poorly understood • Multiple factors within and between patients • Hypotheses: • Presence of antibiotic resistant non-culturable micro-organisms • Chemical irritation • Intra-ductal reflux and obstruction • Dysfunctional high pressure voiding • Neuropathic pain • Pudendal nerve entrapment • Autoimmune
Classification- NIH/EAU • Cat I Acute bacterial prostatitis • Cat II Chronic bacterial prostatitis • Cat III Prostate Pain Syndrome (CPPS) • Cat IV Asymptomatic inflammatory prostatitis
Classification- NIH/EAU • Cat I Acute bacterial prostatitis • Cat II Chronic bacterial prostatitis • Cat III Prostate Pain Syndrome (CPPS) Discomfort or pain in the pelvic region for at least 3 months with variable voiding and sexual symptoms, no demonstrable infection. IIIa- inflammatory PPS- white cells in semen/eps/post eps urine IIIb- non-inflammatory • Cat IV
Evaluation • 3 main factors: • Symptoms • WBC’s • Bacteria
Evaluation • History • Focused Examination • Condition Specific Questionnaires • Urinalysis and Culture • Semen culture • Optional: PSA, Urinary Cytology, US, Cystoscopy, Urodynamics, Psychosocial evaluation
Evaluation • History • Focused Examination • Condition Specific Questionnaires • Urinalysis and Culture • Semen culture • Optional: PSA, Urinary Cytology, US, Cystoscopy, Urodynamics, Psychosocial evaluation
Evaluation • History • Focused Examination • Condition Specific Questionnaires • Urinalysis and Culture • Semen culture • Optional: PSA, Urinary Cytology, US, Cystoscopy, Urodynamics, Psychosocial evaluation
Evaluation • History • Focused Examination • Condition Specific Questionnaires • Urinalysis and Culture • Semen culture • Optional: PSA, Urinary Cytology, US, Cystoscopy, Urodynamics, Psychosocial evaluation
Evaluation IPSS Chronic Prostatitis Symptom Index
Evaluation • History • Focused Examination • Condition Specific Questionnaires • Urinalysis and Culture • Semen culture • Optional: PSA, Urinary Cytology, US, Cystoscopy, Urodynamics, Psychosocial evaluation
Evaluation • Meares-Stamey ‘4 Glass Test’ • 1st 10-15ml of voided urine VB1 • MSU 10-15ml urine VB2 • Prostate Massage- EPS • 1st 10-15ml voided urine post massage VB3 • Modified: VB1 and VB3
Evaluation • History • Focused Examination • Condition Specific Questionnaires • Urinalysis and Culture • Semen culture • Optional: PSA, Urinary Cytology, US, Cystoscopy, Urodynamics, Psychosocial evaluation
Evaluation • History • Focused Examination • Condition Specific Questionnaires • Urinalysis and Culture • Semen culture • Optional: PSA, Urinary Cytology, US, Cystoscopy, Urodynamics, Psychosocial evaluation
Evaluation ‘Diagnosis of exclusion’
Pathogenesis simple Traditional Organcentric Model
Pathogenesis simple Traditional Organcentric Model Infection ‘itis’ Inflammation PAIN!
Pathogenesis simple Antibiotics Anti-inflammatories Alpha blockers Treatment simple? Traditional Organcentric Model Infection ‘itis’ Inflammation PAIN!
Antibiotics • Ciprofloxacin, ofloxacin, levofloxacin • ~10% patients will have culturable bacteria. • J Urol. 2001 May;165(5):1539-44. Predictors of patient response to antibiotic therapy for the chronic prostatitis/chronic pelvic pain syndrome: a prospective multicenter clinical trial. Nickel JC et al. • However, 57% of patients on ofloxacin saw improvement • Trial 2 weeks and continue for 6 if benefit.
Alpha-blockers • Alfuzosin, Terazosin, Tamsulosin • N Engl J Med. 2008 Dec 18;359(25):2663-73. Alfuzosin and symptoms of chronic prostatitis-chronic pelvic pain syndrome Nickel JC et al. • Multicenter, randomized, double-blind, placebo-controlled trial of alfuzosin. • 272 men were randomly assigned to treatment for 12 weeks with either 10 mg of alfuzosin/day or placebo. • The primary outcome was a reduction of at least 4 points in the CPSI score.
Anti-inflammatories • Celecoxib, rofecoxib • J Urol. 2003 Apr;169(4):1401-5. A randomized, placebo controlled, multicenter study to evaluate the safety and efficacy of rofecoxib in the treatment of chronic nonbacterial prostatitis. Nickel JC et al. • Multicenter, randomized, double-blind, placebo-controlled trial of rofecoxib. • 161 men were randomly assigned to treatment with either 25-50 mg of rofecoxib/day or placebo. • Of the patients, 79% on 50 mg rofecoxib versus 59% on placebo reported no or mild pain. But not statistically significant.
Neuropathic Painkillers • Amitriptylline, Pregabalin • Arch Intern Med. 2010 Sep 27;170(17):1586-93. Pregabalin for the treatment of men with chronic prostatitis/chronic pelvic pain syndrome: a randomized controlled trial. Pontari MA et al. • Multicenter, randomized, double-blind, placebo-controlled trial of pregabalin. • 218 men were randomly assigned to treatment for 6 weeks with either 150-600 mg of pregabalin/day or placebo. • The primary outcome was a reduction of at least 6 points in the CPSI score.
So are we getting desperate? • Laparoscopic prostatectomy for chronic prostatitis This study is currently recruiting participants. Verified by the Krongrad Institute Oct 2008. ClinicalTrials.gov identifier: NCT00775515
UPOINT Urinary Tenderness Psychosocial Neurogenic/Systemic Organcentric Infection
UPOINT • Retrospective study of 90 CPPS patients seen by one Urologist over 12 months
Novel Therapies • Cernilton • Eur Urol. 2009 Sep;56(3):544-51. A pollen extract (Cernilton) in patients with inflammatory chronic prostatitis-chronic pelvic pain syndrome: a multicentre, randomised, prospective, double-blind, placebo-controlled phase 3 study. Wagenlehner FM et al. • Multicentre, prospective, randomised, double-blind, placebo-controlled trial in men with CP/CPPS (NIH IIIA) • Primary end-point, defined as a decrease of the CPSI total score by at least 25% or at least 6 points.
Take Home Points • Poorly understood aetiology/pathogenesis. • Heterogenous disease. • Established treatments perform poorly in RCT’s. • Phenotyping patient and treatment. • ‘Active exclusion, Active Inclusion’