Download
1 / 75
760 likes | 1.07k Views
Expectations Vs Achievements - Quality Control Of Blood Components. Sitalakshmi S Professor and Head Department of Clinical P athology St John’s Medical College, Bangalore. The Case…….

E N D
Expectations Vs Achievements - Quality Control Of Blood Components Sitalakshmi S Professor and Head Department of Clinical Pathology St John’s Medical College, Bangalore
The Case……. • A 65-year old lady, was referred to the Medical College Hospital for recent onset fatigue and weight loss . • A CBC showed a WBC count 55,000/ul with 90 % peroxidase positive blasts, normochromic normocytic anemia (Hgb 8 g/dl) and thrombocytopenia (40,000/ul).
On physical exam, the patient was afebrile, normotensive • There were no bleeding manifestations • An admission ECG and history are negative for cardiovascular disease
Need for transfusion? • Does the patient require transfusion of: packed red blood cells? platelets? • Although the patient is mildly anemic and thrombocytopenic, she does not fulfill criteria for transfusion at this time. • Her Hgb > 7g/dl with no history of cardiovascular disease or symptomatic anemia (other than fatigue).
If the patient had a history of cardiovascular illness or signs or symptoms of significant anemia, it would be appropriate to maintain her Hct at a higher baseline. • Similarly, the patients platelet count (40,000/ul ) with no bleeding manifestations does not require prophylactic platelet transfusion
Further Clinical Course…. • Eight days after admission for induction chemotherapy, the patient's CBC shows:WBC 500/ulHgb 6.9g/dl Platelet 8,000/ulThe patient's physician ordered 2 units leukoreduced and irradiated packed red blood cells and 6 units of pooled platelet concentrates (3 X 10¹¹ platelets total). Was transfusion of PRBC and platelets appropriate in this patient at this time?
Need for transfusion….. • Yes. The patient's hemoglobin < 7.0 g/dL in the setting of a bone marrow failure • Likewise, the patient's platelet count has now decreased to the point where she is at risk for spontaneous hemorrhage
A CBC 1 hour after the administration of platelets and PRBC shows:Hgb 9.1g/dl Hct 27.3 % Platelets 30,000/ul Corrected count increment (CCI)(postTPC - preTPC) x (BSA in M²)/(TNPTx 10¹¹) where: TPC=transfusion platelet count BSA=body surface area TNPT=total number of platelets transfusedFor this patient: post TPC 30,000 pre TPC 8,000 CCI=(30-8) x 1.5/3 = 11
Did the patient get an appropriate response from the PRBC and platelet transfusions? Yes to both. The patient was transfused with 2 units of packed red cells (PRBC), Hgb of 6.9g/dl rising to 9.1g/dl. An average adult show a 1 g or 3% rise in Hct with each unit of packed red cells. Likewise, the calculated CCI was 11.0. A CCI of > 7.0 is considered a good clinical response.
What are the factors that affect the patient’s response to transfusion of blood components?
Quality of blood components transfused • Patient’s disease condition and patients physiological response to transfusion • How do we as transfusion specialists ensure quality of blood components? • What is our role in patient transfusion therapy?
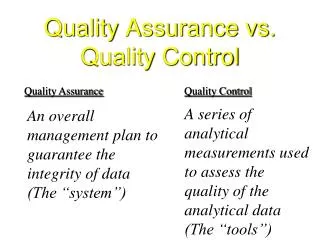
Quality programmes and systems in transfusion medicine differ slightly from other disciplines of laboratory medicine • It takes two different forms. • the blood supply systemand • Clinical transfusion therapy.
The approach used to ensure highest quality in the blood supply system is similar to that used in the manufacture of pharmaceuticals • The approach used to ensure that the patient receives highest quality of transfusion therapy is a part of hospital’s overall quality care program
The measures taken for quality assurance in transfusion medicine are: • Measures needed during the process of blood component preparation and storage • Measures taken during the process of actual transfusion of the blood components. This aspect has more to do with good clinical transfusion practices
Standards for Quality monitoring • The wide variability of the source material from which blood components are prepared makes it difficult to set stringent limits. • Nevertheless, realistic minimum specifications should be set and complied with.
Standards for quality monitoring • The standards are based on minimum requirements • On what is achievable using the most up-to-date methods and systems • Testing of random components to ensure they achieve reliably minimum specific requirements as per the standards
Component preparation • The quality of the components is assured by control of all stages of manufacture • donor selection • Blood collection • Component separation • labeling • Storage
The starting materials for preparation of blood components are blood donations collected from suitable donors. • Conditions of storage or transport • and the time prior to processing, • are contributing factors to the quality of the product.
Delays in preparation • unsuitable conditions of storage or transport • may adversely affect the quality of the final product. • Blood and blood components should be placed in controlled and validated conditions as soon as possible after collection.
Quality assurance is concerned with every aspect of transfusion practice and applied to all activities of blood transfusion service from: QUALITY ASSURANCE Identification of suitable Blood donors Collection of blood Preparation of blood components Blood transfusion
Srandard Operating procedures • The standard operating procedures should describe the specifications for materials that will influence the quality of the final blood component. • Specifications should be in place for blood components (intermediate and final components), starting materials, additive solutions, blood collection bags and equipment.
Blood Collection • The collection process itself is crucial for the quality of blood components. • Measures such as a reliable arm-cleaning and disinfection procedure, the use of closed and sterile collection systems should be implemented. • Free flow of blood during collection is crucial • Time limits is defined for the processing of blood components.
Each component should be visually inspected at each stage of processing and immediately prior to issue. • The component must be withdrawn if there is evidence of leakage, damage to or fault in the container, excessive air, suspicion of microbial contamination or any other contraindications such as platelet clumping, unusual turbidity, haemolysis or other abnormal colour change.
Frequency of quality control • Should be performed on • at least 1% of all components produced • for all parameters to be measured • If fewer than 100, then at least 4 per month • 75% or more of components monitored must meet • the specifications
Transport • Donations and samples should be transported to the processing site in accordance with procedures that ensure a constant approved temperature. • This is especially important when blood is transported from distant collection sites. • Portable temperature loggers may be used to record the temperature during the transportation of blood to the processing site.
Component weight: volume • To provide information, which is useful for clinicians, the component specifications generally require the component label to indicate a volume. • whole blood volume is calculated by deducting the weight of the bag assembly and dividing the resulting weight by the specific gravity of 1.06
Component weight: volume • For red cell components, volume is calculated by weighing the pack, deducting the weight of the pack assembly only and dividing the resultant weight by the specific gravity 1.09 • For platelets and plasma components, volume is calculated by weighing the pack, deducting the weight of the pack assembly and dividing the resulting weight by the specific gravity of 1.03.
Standard Operating procedures • The standard operating procedures for component preparation should be followed at all times using the validated methods. • Any deviations from these established procedures and processes may result in products not meeting specifications and such products should be considered as non-conforming products and must not be released .
Methods of production • Blood components may be prepared by using a centrifugation step with subsequent separation, or by apheresis technology during collection • The use of closed systems is a must for all steps in component processing. • Where sterile connecting devices are used to maintain a functionally closed system they should be correctly used in accordance with a validated procedure. The resulting weld should be checked for satisfactory alignment and integrity.
Equipment • Equipment used in collection, processing, testing and storage of blood and blood component should be observed, standardized and calibrated on a regularly scheduled basis • Procedures should be described in the Standard Operating Procedure (SOP) Manual
Refrigerated centrifuge • Calibrated upon installation and repair • Calibration of speed with tachometer twice a year • Timer to be checked with tachometer
Platelet agitator • Number of strokes 70+/- 10 per min • Periodic cleaning and lubrication
Quality Control of equipment for component storage • Daily periodic temperature monitoring of refrigerators, freezers and platelet incubator • Temperature check at different locations in large equipment • Audio and visual alarms to alert • Continuous temperature recorder • Actual temperature checked with Hg themometer in glycerol
centrifugation • The centrifugation parameters (revolutions per minute, temperature, time, acceleration, deceleration) are important for the composition and characteristics of the specific components. • These critical parameters should be defined on the basis of validation data that demonstrate a process that consistently produces quality products. • For each run, the centrifugation records should identify the operator and confirm that the centrifugation process was performed according to specifications.
Separation • After centrifugation, the bag system should be carefully removed from the centrifuge and placed into a plasma expressor or blood separation system. • The different layers of the components (red cells, platelets, plasma) should be transferred to the satellite bags within the closed systems, in a manner designed to optimize the harvest of the intended component while minimizing the carry-over of other component fractions. • Alternatively, blood components can be separated during collection by apheresis technology
Packed Red cell concentrate • Red-cell concentrates are obtained from whole blood by centrifugation and removal of plasma with or without buffy coat, depending on the centrifugation parameters. • The red cells should be stored at 2–6°C as soon as possible. Alternatively, red-cell concentrates may be obtained using an apheresis system and stored at 2–6°C.
leucoreduction • To obtain leukocyte-reduced red-cell concentrates, either whole blood filtration can be applied prior to separation or there can be a post-separation filtration of the red-cell concentrate.. • Red-cell concentrates are stored at 2 -8oC. The storage time depends on the anticoagulant/preservative solution used. • The introduction of any leukocyte reduction process either by filtration or special centrifugation technique requires careful validation
leucoreduction • Counting residual WBC by automated cell counters may not be reliable for very low WBC count of < 100WBC /ul • Nageotte counting chambers are reliable for as low as 1 WBC/ul • Flow cytometer can detect as low as 0.1 WBC/ul
Further methods of preparation, such as irradiation or washing, are applied to obtain specific red-cell products, depending on the clinical indication. • Periodic quality control should be performed on the final product to ensure that the manufacturing process is consistent At a minimum, the following critical parameters should be checked during the quality control assays: — volume — haematocrit — haemolysis at the end of storage — residual leukocytes, if leukocyte reduction is performed.
Freezing of plasma • Freezing is an important processing step that has an impact on quality of plasma. The rate at which freezing proceeds and the core temperature are both important parameters. • Freezing speed will be influenced by the the freezing equipment, loading pattern and the volume of plasma. • Rapid plasma freezing prevents or reduces the loss of critical constituents such as Factor VIII in frozen plasma.
Fresh Frozen Plasma • FFO is prepared either from whole blood or from plasma collected by apheresis, and is frozen within a defined period of time to a temperature that should adequately maintain the labile coagulation factors in a functional state. • Factor VIII content is critical both as a quality indicator and to assure the efficacy of cryoprecipitate. • If plasma is separated from a unit of whole blood that is refrigerated to 4°C, centrifugation should preferably take place within eight hours of collection
Platelet concentrates • Platelet concentrates are derived from whole blood or are obtained by apheresis. • After collection, whole blood can be kept at 20°C and 24°C,. for up to 4 – 6 hours • The whole blood unit is centrifuged so that an optimal number of platelets remain in plasma (platelet-rich plasma, or PRP). Platelet concentrates are then obtained by hard-spin centrifugation of PRP and are then resuspended.
Platelet concentrates • if whole blood is centrifuged so that the blood platelets are primarily sedimented to the buffy coat layer, the buffy coat is separated and further processed to obtain a platelet concentrate. • Either a single buffy coat or a pool of buffy coats is diluted with plasma, and platelets are concentrated by further centrifugation. • The platelet content per unit depends on the method of preparation. Similarly, the residual leukocyte content will vary according to the centrifugation parameters
Platelet concentrates (both from whole blood and apheresis) should be stored in conditions that guarantee that viability and haemostatic activities are optimally preserved. • The storage temperature should be 20–24°C. • Continuous gentle agitation of platelets during storage should be sufficient to guarantee the availability of oxygen to the platelets (but should be as gentle as possible). • A storage time should not exceed five days