Download
1 / 42
420 likes | 617 Views
Chapter 18: The Shoulder Complex. The shoulder is an extremely complicated region of the body Joint which has a high degree of mobility but not without compromising stability

E N D
The shoulder is an extremely complicated region of the body • Joint which has a high degree of mobility but not without compromising stability • Involved in a variety of overhead activities relative to sport making it susceptible to a number of repetitive and overused type injuries • Movement and stabilization of the shoulder requires integrated function of the rotator cuff muscles, joint capsule and scapula stabilizing muscles
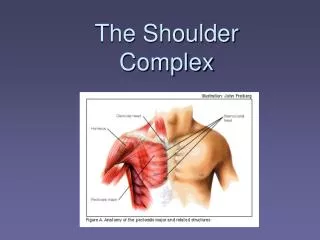
Functional Anatomy • Sternoclavicular (SC) joint • Clavicle articulates with manubrium of the sternum • Weak bony structure but held by strong ligaments • Fibrocartilaginous disk between articulating surfaces • Shock absorber and helps prevent displacement forward • Clavicle permitted to move up and down, forward and backward and in rotation • Clavicle must elevate 40 degrees to allow upward rotation of scapula and thus shoulder abduction
Functional Anatomy • Acromioclavicular (AC) Joint • Lateral end of clavicle with acromion process of scapula • Weak joint and susceptible to sprain and separation • AC ligament, CC ligament, & thin fibrous capsule • Posterior rotation of clavicle as arm elevates • Must rotate approx. 50 degrees for full elevation to occur
Functional Anatomy • Coracoacromial arch • Arch over the GH joint formed by coracoacromial arch, acromion and coracoid process • Subacromial space: area in between CA arch and humeral head • Supraspinatus tendon, long head biceps tendon, and subacromial bursa • Subject to irritation and inflammation as a result of excessive humeral head translation or impingement from repeated overhead activity
Glenohumeral (GH) Joint • Ball and socket, synovial joint in which round head of humerus articulates with shallow glenoid fossa of scapula • stabilized slightly by fibrocartilaginous rim called the Glenoid Labrum • Humeral head larger than glenoid fossa • At any point during elevation of shoulder only 25 to 30% of humeral head is in contact with glenoid • Statically stabilized by labrum and capsular ligaments • Dynamically stabilized by deltoid and rotator cuff muscles
Scapulothoracic (ST) Joint • Not a true joint, but movement of scapula on thoracic cage is critical to joint motion • Scapula capable of upward/downward rotation, external/internal rotation & anterior/posterior tipping • In addition to rotating other motions include scapular elevation and depression & protraction (abduction) and retraction (adduction)
ST Joint • During humeral elevation (flexion, abduction and scaption) scapula and humerus must move in synchronous fashion • Often termed scapulohumeral rhythm • Total range 180°: 120° @ GH joint, 60° of scapular mvmt • Ratio of 2:1, degrees of GH movement to scapular movement after 30 degrees of abduction and 45 to 6 degrees of lfexion • Maintain joint congruency • Length-tension relationship for numerous muscles • Adequate subacromial space
Scapulohumeral rhythm • During humeral elevation • Scapula upwardly rotates • Posteriorly tips • Externally rotates • Elevates • & Retracts • Alterations in these movement patterns can cause a variety of shoulder conditions
Stability of shoulder joint • Instability often the cause of many specific shoulder injuries • During movement essential to maintain position of humeral head relative to glenoid • Likewise it is essential for glenoid to adjust its position relative to moving humeral head, while maintaining stable base
Rotator cuff muscles along with long head of the biceps provide dynamic stability • control the position of humeral head • Prevent excessive displacement or translation of humeral head relative to glenoid • Co-activation of rotator cuff muscles function to compress humeral head into glenoid for stability, as well as depress humeral head • counteracts contraction of deltoid which is elevating humeral head • Imbalance between muscle components will create abnormal GH mechanics and injury
Scapular stability and mobility • Scapular muscles play critical role in normal function of shoulder • Produce movement of scapula on thoracic cage • Dynamically position glenoid relative to moving humerus • levator scap & upper trap=scap elevation • middle trap & Rhomboids=scap retraction • Lower trap=scap retraction, upward rotation and depression • Pec minor=scap depression • Serratus anterior=scap abduction and upward rotation • Only attachment of scapula to thorax is through these muscles
Prevention of Shoulder Injuries • Proper physical conditioning is key • Develop body and specific regions relative to sport • Strengthen through a full ROM • Focus on rotator cuff muscles in all planes of motion • Be sure to incorporate scapula stabilizing muscles • Enhances base of function for glenohumeral joint
Warm-up should be used before explosive arm movements are attempted • Contact and collision sport athletes should receive proper instruction on falling • Protective equipment • Mechanics versus overuse injuries
Throwing Mechanics • Instruction in proper throwing mechanics is critical for injury prevention
Windup Phase • First movement until ball leaves gloved hand • Lead leg strides forward while both shoulders abduct, externally rotate and horizontally abduct • Cocking Phase • Hands separate (achieve max. external rotation) while lead foot comes in contact w/ ground • Acceleration • Max external rotation until ball release (humerus adducts, horizontally adducts and internally rotates) • Scapula elevates and abducts and rotates upward
Deceleration Phase • Ball release until max shoulder internal rotation • Eccentric contraction of ext. rotators to decelerate humerus while rhomboids decelerate scapula • Follow-Through Phase • End of motion when athlete is in a balanced position
Assessment of the Shoulder Complex • History • What is the cause of pain? • Mechanism of injury? • Previous history? • Location, duration and intensity of pain? • Crepitus, numbness, distortion in temperature • Weakness or fatigue? • What provides relief?
Observation • Elevation or depression of shoulder tips • Position and shape of clavicle • Acromion process • Biceps and deltoid symmetry • Postural assessment (kyphosis, lordosis, shoulders) • Position of head and arms • Scapular elevation and symmetry • Scapular protraction or winging • Muscle symmetry • Scapulohumeral rhythm Insert 18-6
Recognition and Management of Specific Injuries • Clavicular Fractures • Cause of Injury • Fall on outstretched arm, fall on tip of shoulder or direct impact • Occur primarily in middle third (greenstick fracture often occurs in young athletes) • Signs of Injury • Generally presents w/ supporting of arm, head tilted towards injured side w/ chin turned away • Clavicle may appear lower • Palpation reveals pain, swelling, deformity and point tenderness
Clavicular Fractures (continued) • Rehab concerns • Closed reduction - sling and swathe, immobilize w/ figure 8 brace for 6-8 weeks • Possible involvement of AC and SC joints • Clavicle insertion for deltoid, upper trap & pec major • Provide stability and neuromuscular control to shoulder complex • Must be addressed in rehab • Removal of brace should be followed w/ joint mobilization of clavicle, isometrics and use of a sling for 3-4 weeks • AROM & PROM • Occasionally requires operative management
Fractures of the Humerus • Cause of Injury • Humeral shaft fractures occur as a result of a direct blow, or fall on outstretched arm • Proximal fractures occur due to direct blow, dislocation, fall on outstretched arm • Care • Immediate application of splint, treat for shock and refer • Athlete will be out of competition for 2-6 months depending on location and severity of injury • Progressive ROM exercises as tolerated • PRE exercises of shoulder & elbow after 4-6 weeks • Maintain strength of elbow, forearm and wrist musculature
Sternoclavicular Sprain • Cause of Injury • Indirect force, blunt trauma (may cause displacement) • Care • PRICE, immobilization • Immobilize for 3-5 weeks followed by graded reconditioning • Strengthen muscles in range that does not put further stress on joint • Low grade joint mobilizations after inflammation is controlled • Restore normal mechanics of shoulder complex
Acromioclavicular Sprain • Cause of Injury • Result of direct blow (from any direction), upward force from humerus, fall on outstretched arm • Signs of Injury • Grade 1 - point tenderness and pain w/ movement; no disruption of AC joint • Grade 2 - tear or rupture of AC ligament, partial displacement of lateral end of clavicle; pain, point tenderness and decreased ROM (abduction/adduction) • Grade 3 - Rupture of AC and CC ligaments with dislocation of clavicle; gross deformity, pain, loss of function and instability
Care • Ice, stabilization, referral to physician • Grades 1-3 (non-operative) will require 3-4 days (grade 1) and 2 weeks of immobilization ( grade 3) respectively • Aggressive rehab is required w/ all grades • Joint mobilizations, flexibility exercises, & strengthening should occur immediately • Progress as athlete is able to tolerate w/out pain and swelling • Padding and protection may be required until pain-free ROM returns • Grade 1 & 2 often treated conservatively while grade 3 may require surgical intervention to reduce separation although often treated w/o surgery also • Grade IV, V & VI- require internal fixation to realign fractured segments
Glenohumeral Dislocations • Cause of Injury • Head of humerus is forced out of the joint • Anterior dislocation is the result of an anterior force on the shoulder, forced abduction, extension and external rotation • Occasionally the dislocation will occur inferiorly • Signs of Injury • Flattened deltoid, prominent humeral head in axilla; arm carried in slight abduction and external rotation; moderate pain and disability
Care • RICE, immobilization and reduction by a physician • Begin muscle re-conditioning ASAP • Use of sling should continue for at least 1 week • Progress to resistance exercises as pain allows
Shoulder Impingement Syndrome • Cause of Injury • Mechanical compression of supraspinatus tendon, subacromial bursa and long head of biceps tendon due to decreased space under coracoacromial arch • Seen in over head repetitive activities • Signs of Injury • Diffuse pain, pain on palpation of subacromial space • Decreased strength of external rotators compared to internal rotators; tightness in posterior and inferior capsule • Positive impingement and empty can tests
Care • Restore normal biomechanics in order to maintain space • Strengthening of rotator cuff and scapula stabilizing muscles • Stretching of posterior and inferior joint capsule • Modify activity (control frequency and intensity)
Rotator cuff tear • Involves supraspinatus or rupture of other rotator cuff tendons • Primary mechanism - acute trauma (high velocity rotation) • Occurs near insertion on greater tuberosity • Full thickness tears usually occur in those athletes w/ a long history of impingement or instability (generally does not occur in athlete under age 40) • Signs of Injury • Present with pain with muscle contraction • Tenderness on palpation and loss of strength due to pain • Loss of function, swelling • With complete tear impingement and empty can test are positive
Care • RICE for modulation of pain • Progressive strengthening of rotator cuff • Reduce frequency and level of activity initially with a gradual and progressive increase in intensity
Shoulder Bursitis • Etiology • Chronic inflammatory condition due to trauma or overuse - subacromial bursa • May develop from direct impact or fall on tip of shoulder • Signs of Injury • Pain w/ motion and tenderness during palpation in subacromial space; positive impingement tests • Management • Cold packs and NSAID’s to reduce inflammation • Remove mechanisms precipitating condition • Maintain full ROM to reduce chances of contractures and adhesions from forming
Bicipital Tenosynovitis • Cause of Injury • Repetitive overhead athlete - ballistic activity that involves repeated stretching of biceps tendon causing irritation to the tendon and sheath • Signs of Injury • Tenderness over bicipital groove, swelling, crepitus due to inflammation • Pain when performing overhead activities • Care • Rest and ice to treat inflammation • NSAID’s • Gradual program of strengthening and stretching
Contusion of Upper Arm • Cause of Injury • Direct blow • Repeated trauma could result in development of myositis ossificans • Signs of Injury • Pain and tenderness, increased warmth, discoloration and limited elbow flexion and extension • Management • RICE for at least 24 hours • Provide protection to contused area to prevent repeated episodes that could cause myositis ossificans • Maintain ROM
Multi-directional instability • When forces that are generated at GH joint that stabilizing muscles are unable to handle humeral head tends to translate anteriorly and inferiorly • Overtime cause structures to stretch • Increase demands of posterior structures • Eventual breakdown of these tissues
MDI rehab considerations • Emphasis on anterior and posterior musculature • Promote neuromuscular control to assist dynamic stability • Patient must be compliant with exercises to avoid instability and/or repetitive subluxations • Surgical intervention is sometimes required to tighten joint capsule