Download
1 / 41
420 likes | 615 Views
Aphasia Notes. Test III Athena Hagerty. General Info about Treatment:

E N D
Aphasia Notes Test III Athena Hagerty
General Info about Treatment: • Working with Adults: you can tell them what they are doing and why. You can provide concrete feedback to your patient. Telling the person what they are doing a great job at. You can provide feedback for errors. “That wasn’t a good way to say that, tell me again”. Progress is its own reward. Instead of planning for kiddos, adults are happy for therapy, you don’t have to give them a sticker.
General Info about Treatment: • Planning for treatment- don’t take hours, do it easily and it’s cheap or free for therapy. Free newspapers from Dubois. Clinic has a laminator. Paper, pencil and you can do therapy
Generalization: • Loose training- you should consider stimulus items that elicit a variety of acceptable responses. 1 cup for multiple things • Sequential modification- treat in different environments and diff. contexts. • Does Treatment Work? • Aphasia therapy work? YES. But It needs very good guidance from the clinician. Don’t do workbook stuff. If they don’t need you, they shouldn’t be in therapy. Computer programs are bad. Group therapy also WORKS. Evidence behind it. More support by other patients. Maintaining skills.
Goals of Aphasia Therapy • Empowering the patient- you teach them skills that they can use. • Communicative Competence- the person can communicate in ANY context. If you can do this with patient you are a successful SLP. • Who receives treatment?- Initially everyone who has aphasia should receive treatment. • Prognosis- there are some people with really poor prognosis= severe Wernicke’s, severe global, after 3 months following injury. If nothing changes after 3 months that’s bad.
Group therapy- if its available, patient should participate. • Evaluation of cognition- you can evaluate cognition as the person improves IF the neruopsych is good at evaluation. • Neuropsych needs to be experienced.
Treatment of Auditory Comp. • Bottom up model- patient is analyzing sounds to make sense of info. Repeating plate over and over again to make sense of it. • Top down model- begins with an expectation about the the speaker will say. Either confirm or change the action depending on the production. Ex- you’re walking and see a friend hows it going? They say not so good, you keep walking, see you later… then go back and ask them what up.
Treatment of Auditory Comp. • Knowledge based/heuristic process- • general knowledge and intuition to deduce meaning of spoken information. • what to expect when you are ordering at a restaurant.
Treatment of Auditory Comp. • Point to/ show me • Y/N questions • Wh- questions/tell me (simple or complex) what is your name? where are you? Does it snow in July? Do you use an axe to cut the grass? • Following Directions (1-3) can increase up to three steps. (WM component) • Sentence verification- person has to listen to sentence and tell if its true or false. Can make it difficult my adding fake words.
Treatment of Auditory Comp. • Task switching activities- • Discourse comprehension – can they actually answer questions? • Familiar- if its familiar it will be easier. • Length & redundancy-
Goal Writing • Long term goal- 3 components to a goal- every supervisor requires these 3 things. • Performance • Condition- type of cues you are using • Criteria –percentage or trials
Treatment of Auditory Comp. Aud comp long term goal- will vary from facility to facility. Determine goal by hierarchy. End point to whatever facility your in. where we want to get the patient eventually. • ST Goals- small steps to get to the long term goal. Baby step to get to long term goal. Point to show me/ y/n • Biggest LT goal- to comprehend conversation. Ask questions during conversation and keep track of answers. • Ex- patient. Moderate aud comp deficits. Are long term goal would be for academic year. ST- semester. Complex y/n questions.
CUES • Cues- extra help • Verbal- explaining or repeating • Phonemic- it’s a” K” for key. • Visual • Pointing • Gestures • Written • Tactile (touch)- holding their hand. Giving them something to feel or touch.
Percentages Maximum moderate minimum assistance. – Dr Isaki doesn’t like these terms. Doesn’t like 3 out of 4 trials. Likes percentages better. • Mild- 90% of time can do tasks. • Moderate-80% of time • Severe-70% of time • Try and shoot for 20% (increase) of time. • Global aphasia- 30% of time correct- yes you can get them to 50% of the time. • Normal is not 80% of the time. You can write a goal for 100% of time if you think you can do it. Because they were capable before the CVA. • If client hits goal 3 times, you then need to review to goals and revise them.
Goal for Auditory Comp. • GOAL for this client- client will answer complex yes/no question with 95% accuracy given verbal cues. In my methods verbal cues means repetition of questions. • Client will follow 3 step commands with 95% accuracy given visual cues. Visual cues may be pointing to item
Expressive language Treatment • Content Words (nouns more important for Global) • Enhance with nonverbal communication (can live w/out articles & adverbs) • Increase length & complexity- Sub, Verb, Obj • Picture Description- take a picture from the newspaper (Norman Rockwell pics) • Storytelling & retelling • Conversation- most difficult • If you improve anomia, you will improve expressive language
Reading Comprehension Tx. (deficits) • Reading glasses? Do they have glasses? • Surface Dyslexia? Lost direct lexical route and now dependent on phonological route. Ex- sound by sound or letter by letter. • Deep dyslexia- you have lost phonological route, now you’re dependent on whole word recognition.
Reading Comprehension Tx. (deficits) • Letters- can they identify a letter? • Words to pics- matching words to pics • Phrase to pics • Sentence- written questions or matching to pics • Paragraph- written questions, 2 sentences, then 3, short stories • Survival Reading (6th grade level) menu, telephone book
Anomic Tx. • Anomia looks like… • Pauses • Fillers “uh, um” • I don’t know • Ineffective gestures
Anomic Tx. Suggestions for therapy • Naming (Rosenbek,Lapointe & Wertz) Choose at least 3 strategies • Semantic description- start describing its attributes, formulate descriptors to pull out. Cat= furry meow. • Embedding- (good for anomic aphasia) formulate your own sentence, embed the word within the sentence. Cup=”You use a _____ for drinking.” • Synonyms- works for high functioning • Antonyms- not every word has an antonym
Anomic Tx. Suggestions for therapy • Rhyming- “cat” “bat”- looking at things that rhyme to get word. • Sentence completion- high functioning= anomic, conduction. “You drink from a _____.” • Phonemic cues- weird strategy. Everyone around patient uses the prompt “You drink from a c____.” • Writing- if you can’t think of a word, can’t write it. • Gestures- depends on person’s vocab, for high functioning patient • Drawing- depends on person’s vocab, for high functioning patient
Anomic Tx. Suggestions for therapy • Once you DO get word: • practice for a couple of trials (recommend 3). • Also practice at the end of session.
Format (Brookshire) • Hello- (only 5 minutes) where you catch up with your patient. How was your week? Etc. • Accommodation- we are going to work on easier tasks first. • Work- where you concentrate on more difficult tasks. • Cool down- more easier tasks so they can feel good about their performance. • Goodbye- reviewing entire session and progress they were able to show. Summarize abilities
Resource Allocation • Central Pool- a way to think about how your therapy is affecting your client, analyze performance. Can pull out all sorts of language abilities and cognitive processes. • Depends on the demands of the task, you can pull out too many processes from the central pool. If this happens, the client will fail. • Reduce processes if client fails. • Environment can affect performance (noisy, busy, etc.) SIMPLIFY environment • Dr Isaki said to change rooms if the room you’re in is too noisy.
Goals of Aphasia Therapy • 1) want patient to regain as much comm as possible as much as their injury allows and their needs drive them. • 2) teach them to compensate for the skills that they lack. • 3) teach them to be in harmony with their lives.
Preparing someone for lifetime of Aphasia • 1) remember to give fair assessments of prognosis (don’t use word normal) • 2) stress the importance of what remains. (everyone has skills) • 3) Aphasia is a human disorder meaning it not only affects language, but a person’s life and relationship to others. Patients are unchanged at the core.
Preparing someone for lifetime of Aphasia • 4. Never forget you are treating a PERSON w/ Aphasia. Try to resist being everything to the patient. • 5. Learn to be a good listener. We’ll hear all types of info. We have boundaries in our profession, refer out as needed. • 6. Have to trust our patients that they are going to survive and cope and life
Preparing someone for lifetime of Aphasia • 7. We are going to be counseling for comm disorders (not depression). Teach them about Aphasia and words we use. National Aphasia Assoc. has great paperwork. • LISTENING IS IMPORTANT. Silence is OK. Wait for them to say something. Shouldn’t be weird. Listen to their family and friends and ask what concerns they have.
Preparing someone for lifetime of Aphasia • Rosenbeck states “that clinicians that are adequate, treat all people more or less equally. A superior clinicians finds out what each patient wants and needs and determines what is possible.
ADULTS • Easiest population. • Easiest prep time • No stickers & crafts • Don’t need to applaud • Comm is its own reward • If you have superior clinician, will see amazing things in therapy. • Patient will try harder and they continue treatment. • Difficult for them to let you go.
ADULTS cont. • You can point out errors and how to change those errors. • You have built this relationship on trust, support and respect. • It is acceptable to exploit a person’s strengths. • Prepare for generalization- client needs to be on their own. Take client out of therapy and let client do their own thing. Then go back in clinic and talk about it.
A good clinician…. • Can adjust to changes- client will have good days and bad. We should be constantly thinking of hierarchy. • Recognizes when therapy isn’t doing very much • Laughter & crying is OK-sympathizing is OK. • Therapy has an ending. If patient plateaus, maybe it’s time to discharge them. You can say “ you can always come see me”.
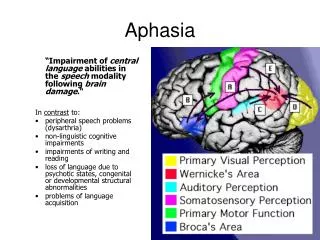
Speech = motor- damage to PMC causes apraxia • Language= syntax semantics etc.
Speech Deficits • Apraxia- the disturbed ability to reproduce purposeful learned movement, despite intact mobility. NO weakness of the musculature. • Ideational Apraxia- the disruption of ideas needed to understand the use of objects. Ex- when we see key, we know how to use it. • Show them object and say “show me how to use it”.
Speech Deficits • Ideomotor Apraxia- requires motor movement. Types of ideomotor: • 1) Buccofacial/nonverbal/oral apraxia- the inability to demonstrate volitional oral movements on command. Exercises on oral mech exam. If you have this apraxia, you’ll see struggle and searching behaviors.
Speech Deficits- type of ideomotor apraxia • 2) Limb Apraxia- inability to demonstrate volitional movements of arm wrist and hand on command. Ex- wave goodbye (they have problems with that). Look for whether they can do movements closer to the body or further away. Assess: if you give them an object they can do movement, take away object, they can’t. Kind of like they can’t pretend.
Speech Deficits- type of ideomotor apraxia • 3) Apraxia of speech- where patient has problems programming the position and sequence of speech musculature, for the production of volitional speech (Darley Def.) • Characteristics: • No weakness or paralysis or sensory loss • Automatic speech is easier than planned speech • Artic consistancies in/of errors. When they make errors it WILL be consistent. • Struggle and searching behavior.
Dysarthrias • Dysarthrias- weakness, paralysis, incoordination of the muscles, required for speech. • Descriptors: speech sounds slurred, unclear, imprecise. • Tx- make sure you have unfamiliar listeners come is to check client’s production because eventually you will understand them after a while.

![[PDF] DOWNLOAD Manual of Aphasia and Aphasia Therapy](https://cdn7.slideserve.com/12535081/slide1-dt.jpg)