Download
1 / 32
320 likes | 633 Views
Aphasia Taskforce. California Association of Superior Court Investigators (CASCI) 2007 Statewide Training Conference John K. Johnson, M.Phil-DPS. Aphasia.

E N D
Aphasia Taskforce California Association of Superior Court Investigators (CASCI) 2007 Statewide Training Conference John K. Johnson, M.Phil-DPS
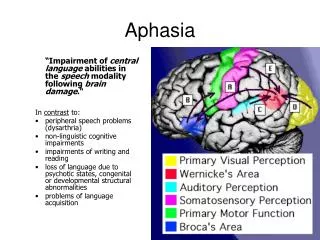
Aphasia Aphasia is a disorder that results from damage to language centers of the brain. For almost all right-handers and for about 1/2 of left-handers, damage to the left side of the brain causes aphasia. As a result, individuals who were previously able to communicate through speaking, listening, reading and writing become more limited in their ability to do so. The most common cause of aphasia is stroke, but gunshot wounds, blows to the head, other traumatic brain injury, brain tumor, and other sources of brain damage can also cause aphasia.
Who has aphasia? Anyone can acquire aphasia, but most people who have aphasia are in their mid to later years. Men and women are equally affected. It is estimated that approximately 80,000 individuals acquire aphasia each year. About one million persons in the United States currently have aphasia.
What causes aphasia? Aphasia is caused by damage to one or more of the language areas of the brain. Many times, the cause of the brain injury is a stroke. A stroke occurs when, for some reason, blood is unable to reach a part of the brain. Brain cells die when they do not receive their normal supply of blood, which carries oxygen and important nutrients. Other causes of brain injury are severe blows to the head, brain tumors, brain infections, and other conditions or trauma of the brain.
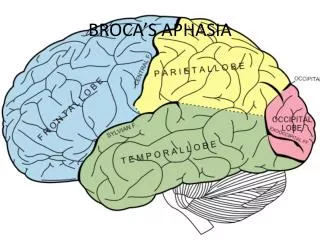
Causes aphasia continued: Individuals with Broca's aphasia have damage to the frontal lobe of the brain. These individuals frequently speak in short, meaningful phrases that are produced with great effort. Broca's aphasia is thus characterized as a “non-fluent” aphasia. Affected people often omit small words such as "is," "and," and "the." For example, a person with Broca's aphasia may say, "Walk dog" meaning, "I will take the dog for a walk." The same sentence could also mean "You take the dog for a walk," or "The dog walked out of the yard," depending on the circumstances.
Causes aphasia continued: Individuals with Broca's aphasia are able to understand the speech of others to varying degrees. Because of this, they are often aware of their difficulties and can become easily frustrated by their speaking problems. Individuals with Broca's aphasia often have right-sided weakness or paralysis of the arm and leg because the frontal lobe is also important for body movement.
Causes aphasia continued: In contrast to Broca's aphasia, damage to the temporal lobe may result in a fluent aphasia that is called Wernicke's aphasia. Individuals with Wernicke's aphasia may speak in long sentences that have no meaning, add unnecessary words, and even create new "words." For example, someone with Wernicke's aphasia may say, "You know that smoodle pinkered and that I want to get him round and take care of him like you want before," meaning "The dog needs to go out so I will take him for a walk."
Causes aphasia continued: Individuals with Wernicke's aphasia usually have great difficulty understanding speech and are therefore often unaware of their mistakes. These individuals usually have no body weakness because their brain injury is not near the parts of the brain that control movement.
Causes aphasia continued: A third type of aphasia, global aphasia, results from damage to extensive portions of the language areas of the brain. Individuals with global aphasia have severe communication difficulties and may be extremely limited in their ability to speak or comprehend language.
How is aphasia diagnosed? Aphasia is usually first recognized by the physician who treats the individual for his or her brain injury. Frequently, this is a neurologist. The physician typically performs tests that require the individual to follow commands, answer questions, name objects, and converse. If the physician suspects aphasia, the individual is often referred to a speech-language pathologist, who performs a comprehensive examination of the person's ability to understand, speak, read, and write.
How do you communicate with an aphasia patient? Some people with aphasia have problems primarily with expressive language (what is said) while others have their major problems with receptive language (what is understood). In still other cases, both expressive language and receptive language are obviously impaired. Language is affected not only in its oral form of talking and understanding but also in its written form of reading and writing.
Communicating with an aphasia patient, continued: Typically, reading and writing are more impaired than oral communication. The nature of the problems varies from person to person depending on many factors but most importantly on the amount and location of the damage to the brain.
Communicating with an aphasia patient, continued: Amount and location of the damage, along with other factors, e.g., age, educational level, and health status, also affect the severity of the problems. Persons with severe aphasia may understand almost nothing of what is said to them and say little or nothing. At best, their oral communication may be only approximations of "yes" and "no" and maybe common social phrases like "hi" and "thanks."
Communicating with an aphasia patient, continued: Persons with mild aphasia may be able to carry on normal conversations in many communication settings. They may have trouble understanding language only when it is long or complex, or they may have some trouble finding the words they need to express an idea or to explain themselves, orally or in written form.
Communicating with an aphasia patient, continued: Word finding problems ( anomia ) are common in people with aphasia and is most like the common experience of having a word "on the tip of our tongues" but not being able to remember it. The person may forget the word comb even though he or she can show you how to use it.
Communicating with an aphasia patient, continued: There are also degrees of aphasia between mild and severe . A person may speak only in single words (e.g., names of objects) or in short, fragmented phrases. Smaller words of speech (e.g., the , of , and ), may be omitted, making the message sound like a telegram. Words may be put in the wrong order and incorrect grammar may be used.
Communicating with an aphasia patient, continued: Sounds and/or words may be switched. A bed may be called a table or a dishwasher a wish dasher . Or, the person with aphasia may make up a word. In some cases, nonsense (or real) words are strung together quite fluently, but make no sense to the listener.
Communicating with an aphasia patient, continued: It usually requires extra effort for the person with aphasia to understand spoken messages, as if he or she is trying to comprehend a foreign language. The person may need extra time to process and understand what is being said by the investigator. It may be especially hard to follow very fast speech like that heard on radio or television news. He or she may misinterpret subtleties of language, e.g., taking the literal meaning for a figure of speech like He kicked the bucket.
Communicating with aphasia patient, continued: Difficulty with one or more of the aforementioned skills may lead to communication breakdowns and frustrating communication for both the person with aphasia and the investigator.
How is aphasia treated? In some instances an individual will completely recover from aphasia without treatment. This type of "spontaneous recovery" usually occurs following a transient ischemic attack (TIA), a kind of stroke in which the blood flow to the brain is temporarily interrupted but quickly restored. In these circumstances, language abilities may return in a few hours or a few days. For most cases of aphasia, however, language recovery is not as quick or as complete.
How aphasia is treated, continued: While many individuals with aphasia also experience a period of partial spontaneous recovery (in which some language abilities return over a period of a few days to a month after the brain injury), some amount of aphasia typically remains. In these instances, speech-language therapy is often helpful. Recovery usually continues over a 2-year period.
How aphasia is treated, continued: Most people believe that the most effective treatment begins early in the recovery process. Some of the factors that influence the amount of improvement include the cause of the brain damage, the area of the brain that was damaged, the extent of the brain injury, and the age and health of the individual. Additional factors include motivation, handedness, and educational level.
How aphasia is treated, continued: Aphasia therapy strives to improve an individual's ability to communicate by helping the person to use remaining abilities, to restore language abilities as much as possible, to compensate for language problems, and to learn other methods of communicating.
How aphasia is treated, continued: Treatment may be offered in individual or group settings. Individual therapy focuses on the specific needs of the person. Group therapy offers the opportunity to use new communication skills in a comfortable setting. Stroke clubs, which are regional support groups formed by individuals who have had a stroke, are available in most major cities.
How aphasia is treated, continued: These clubs also offer the opportunity for individuals with aphasia to try new communication skills. In addition, stroke clubs can help the individual and his or her family adjust to the life changes that accompany stroke and aphasia. Family involvement is often a crucial component of aphasia treatment so that family members can learn the best way to communicate with their loved one.
How Can we as Investigators Communicate with Aphasia Subjects? Follow these simple suggestions:
Investigator’s should: • Simplify language by using short, uncomplicated sentences. • Repeat the content words or write down key words to clarify meaning as needed. • Maintain a natural conversational manner appropriate for an adult. • Minimize distractions, such as a blaring radio, or TV whenever possible. • Include the person with aphasia in conversations when interviewing others in the area.
Investigator’s should: • Ask for and value the opinion of the person with aphasia, especially regarding legal matters. • Encourage any type of communication, whether it is speech, gesture, pointing, or drawing. • Avoid correcting the individual's speech. • Allow the individual plenty of time to talk.
Where can I get additional information? American Speech-Language-Hearing Association (ASHA) 10801 Rockville PikeRockville, MD 20852Voice: (301) 897-5700Toll-free Voice: (800) 638-8255TTY: (301) 897-0157Fax: (301) 571-0457E-mail: actioncenter@asha.orgInternet: www.asha.org
Where can I get additional information? Brain Injury Association of America 8201 Greensboro Drive, Suite 611McLean, VA 22102Voice: (703) 761-0750Toll-free Voice: (800) 444-6443Fax: (703) 761-0755E-mail: info@biausa.orgInternet: www.biausa.org
Where can I get additional information? National Aphasia Association (NAA) 7 Dey Street, Suite 600New York, NY 10007Voice: (212) 267-2814Toll-free Voice: (800) 922-4622Fax: (212) 267-2812E-mail: naa@aphasia.orgInternet: www.aphasia.org