Download
1 / 72
820 likes | 1.35k Views
Participate in the Implementation of Individualised Care Plans. Aims and Objectives. Plan work activities according to an individualised plan Establish and maintain appropriate relationships with clients and carers Provide and monitor support according to the individualised plan

E N D
Participate in the Implementation of Individualised Care Plans
Aims and Objectives • Plan work activities according to an individualised plan • Establish and maintain appropriate relationships with clients and carers • Provide and monitor support according to the individualised plan • Contribute to ongoing relevance of the individualised plan • Respond to situations of risk to the client within work role and responsibilities • Complete documentation and reporting
Organisational policies and procedures • Policies set out the general standards of service for that agency to achieve- must be accessible to all staff, clients and other interested parties. • Procedures are specific written instructions that explain what a staff member is to do, step by step in a particular situation. • It is YOUR responsibility to be familiar with the P & P within your work
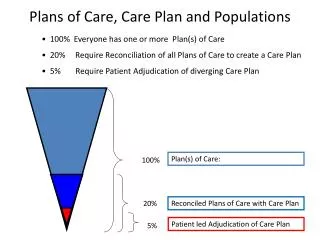
Individualised Plans • Also called Care Plans, Service plans, Client plans. • A care plan is an individualised plan of care and gives directions for staff to follow in the provision of care. • The plan details the care requirements that a person needs on a daily basis. This type of document is generally used in long term care because it replaces the need to detail all care given each day in the resident’s case notes.
Individualised Plans • Provide an accurate, concise notation of the residents’ current condition. • The care plan provide information about the resident’s goals and care needs. • The care plan is a recipe about how the care needs to be provided. • The notes provide baseline information on which to record any improvement or deterioration in the resident’s condition.
Individualised plans • The record provides evidence of care. The records will provide information about what care was provided, by whom, when and any comments from the resident, doctor, or significant other. • The care plan is a dynamic document, meaning that it changes regularly dependent on the needs and changes in the resident. It should be used and reviewed on a regular basis. The care plan is a care tool to direct and guide staff in how the care needs to be provided to the resident. • Care plans need to be individually tailored to the care needs of the individual, there is no magic formula to suit all residents, however there are some basic guidelines which you can follow in order to formulate the care plan.
The Nursing Process and Care Planning • Assessment • Planning • Implementation • Evaluation
Assessment • Observation of their needs by sight, hearing, touch and smell • • Communication with other members of the team to make accurate assessment of the care needs of the resident. Sometimes care workers need to provide different care activities to the same resident. Either because the resident favours a particular care worker of that the worker has expert knowledge.
Assessment • A thorough assessment must be compiled in a variety of areas to determine the long term care needs and goals of client care. Areas of assessment include the following: • Physical care needs • Psychological care requirements • Socialisation needs of the individual • Spiritual needs • Assistance to maintain their personal affairs • Relationships with family and others
Personal profile Communication Assessment Social and emotional needs assessment Nutrition and Hydration Assessment Mobility Assessment including falls risk and manual handling assessments Personal hygiene assessments, physical assessments oral hygiene assessments Toileting assessments Continence assessments Bladder and bowel Psychogeriatric Assessment scale (PAS) Behaviour Assessment – Verbal, Wandering, Physical agitation Cornell depression scale Medication Assessments Complex care needs Assessments – Pain scales, Waterlow scale for skin integrity, diabetes Assessment etc Assessment forms currently used
Planning • Once the assessment is completed goals of care need to be developed. The goals determine whether a client will be able to restore or maintain their current level of care. The goal of care may be to improve the person’s current ability or simply to preserve their current function and level of independence.
Sample Care Plan • Impaired Verbal Communication • Identified need/Problem: • Impaired verbal communication related to: • Decreased oxygen to the brain. • Unable to speak English • Impaired articulation. • Disorientation. • Loose association of ideas, • Inability to speak sentences. • Slur or stutter.
Sample care plan • Goal: • Resident will communicate and participate in activities of daily living using either verbal or non verbal modes. Assess contributing factors. Note whether the problem is expressive (loss of speech), Sensory (unable to understand words, Conduction (slow comprehension) or Global (loss of comprehension and speech).
Implementation • The nurses actions • Like a written handover, how everyone should be carrying out the care. • Ensures that everyone is doing the same level of care
Sample care plan Interventions: •Determine native language spoken and cultural background. • Assist patient to establish means of communication. • Listen carefully to patient on verbal expressions. • Validate meaning of non-verbal communication. • Maintain eye contact. • Keep communication simple. • Plan for alternative methods of communication (written instructions or picture boards). • Maintain a calm unhurried manner- allowing time for the resident to respond.
Evaluation • This includes your monthly, two monthly evaluation of how the person r the care is meeting their goals and preferences • It assists to determine if the staff are meeting the needs of the client.
Evaluation • See ACFI Checklists
What are the Care Worker responsibilities • READ the individualised care plans • Evaluate them regularly • Input into the care plans from your individual knowledge of the client • Contribute to case conferences and feed back the effective actions you use
Communication • Introducing yourself • With client • With staff • With management • With relatives and friends • Documentation
Introducing yourself • Be polite. • Use open communication skills. • Be genuine in your motivation. • Provide name, position and the task you want to carry out. • Wait until you have consent. • Respect the person’s right to refuse. • Check your own emotions, feelings, frustrations before you enter the room.
Communication with clients • Respect basic human rights • Be approachable • Sometimes need to make the first move to communicate • Develop a trusting relationship • Clear, calm, open language and body language. • Be culturally sensitive. • Allow clients to make as many decisions as they can.
Communication with staff • Be understanding of the mood/stress of other staff • Be willing to work with them • Use the “power with” not the “power over” principle • Be willing to learn from others, instead of right every time. • Work cooperately, plan and talk all shift.
Communication with Management • Understand that reporting on is part of your job role. • Find convenient times to report. • How urgent is the incident/ problem? • Give your opinion in an appropriate setting. • Be respectful of the position your manager holds. • Provide clear communication or written documentation.
Communication with Relatives and Friends • Find out the policy on what you can communicate and who can communicate the information. • Develop a rapport with relatives but do not breach confidentiality. • Communicate what your job role allows but do not communication information outside of your scope of practice.
Confidentiality and Privacy • Personal information, which is obtained while caring for a client, is confidential. The client has the right to decide who to share this information with. Confidentiality applies to information that a client or other care worker tells you verbally or gives you in writing. It also applies to things that you learn through observation. All information in a person’s health care record is confidential and may not be disclosed without permission from the client or their guardian. Information may be shared with other relevant health and aged care workers when they need the information in order to provide appropriate care.
Maintaining Confidentiality A carer has a moral duty and often legal obligation to protect the privacy of an individual by restricting information obtained in a professional capacity to appropriate personnel and settings, and to professional purposes. A nurse must, where relevant, inform an individual that in order to provide competent care, it is necessary for a carer to disclose information that may be important to the clinical decision making by other members of a health care team. A carer must, where practicable, seek consent from the individual or a person entitled to act on behalf of the individual before disclosing information. In the absence of consent, the nurse uses professional judgement regarding the necessity to disclose particular details, giving due consideration to the interests, well–being, health and safety of the individual and recognising that the carer is required by law to disclose certain information.
Privacy • In the context of Aged care and Health care privacy means discretion and secrecy
Appropriate conversation • Need to socially appropriate at all time. • Need to direct your conversation at the clients needs or carers needs- NOT YOUR OWN. • Do not swear, complain, or give out personal or sensitive information. • Be friendly with your work mates but remember they are not your best friend. • Do not reveal personal information to colleagues.
1. Define the problem 2.Generate Ideas 3. Investigate solutions 4. Choose an option 5.Plan to act 6. Evaluation Problem solving skills
Use the problem solving technique to solve the following problem • The co-worker that you are teamed with likes to spend time talking to the clients, and leaves you the bulk of work. • It also means that you have trouble getting to know the clients you work with. • What could you, and your work team, do to resolve this situation?
Providing care • Assessment • Observation • Questioning • Consultation • Medical History • Physical ability • Lifestyle choices • Family history and dynamics • Past experiences • Social contacts
Role of an Aged Care Worker • Multi skilled • Flexible in work practices in care delivery • Work as part of the multi-disciplinary team • Participate in planning & delivery of care • Abide by the mission statement & job description • Responsibilities include- OHS, documentation, provision of care.
Role & Responsibility • To observe (collect physical data) the patient; • Report to supervisor/ RN any change in a pts condition; • Other areas the AIN is responsible for reporting include: equipment faults, safety hazards, need for supplies, incidents/ accidents, breaches in confidentiality, absences from duty/ breaches in duty of care- abuse.
What is expected of you as an AIN • Fulfils the duties of the job description • Technical skills (i.e.. BP) communication skills (interaction with staff & clients) • Time management • Team work • Documentation skills
Conscientious Trustworthy Patient Thorough cooperative Respectful Caring Honest Accurate Empathetic Reliable Flexible Organised Adaptable Flexible Passionate Personal attributes
Rights of workers • Safe work environment • Free from harassment and discrimination • Work conditions and wages in accordance with IR laws • EEO
Accountability & Responsibility • Duties as per job description • Completion of specific tasks at the required standard in a reasonable time frame. • Accountable means you are answerable for the things you do. • Who are you accountable and responsible to?
Activity • Think of an organisation you know and develop an Organisational chart which indicates who you report to.