Download
1 / 31
350 likes | 873 Views
Coronary Atherosclerosis . Prepared by Wala’a Fathi Abed Al Fatah Hassan. Definition. Is a disease affecting the arterial blood vessel, it is commonly referred to as a "hardening" or "furring" of the arteries. It is caused by the formation of multiple plaques within the arteries.

E N D
Coronary Atherosclerosis Prepared by Wala’a Fathi Abed Al Fatah Hassan
Definition Is a disease affecting the arterial blood vessel, it is commonly referred to as a "hardening" or "furring" of the arteries. It is caused by the formation of multiple plaques within the arteries. Basically it is characterized by intimal plaques called "atheromas".
Pathologically The atheromatous plaque is divided into three distinct components:- 1.The atheroma:- is the nodular accumulation of a soft, flaky, yellowish material at the center of large plaques, composed of macrophages nearest the lumen of the artery. 2. The underlying areas of cholesterol crystals, and possibly also. 3. Calcification at the outer base of older/more advanced lesions.
Pathogenesis 1-The development of focal areas of chronic endothelial injury, usually subtle, with resulting increased endothelial permeably or other evidence of endothelial dysfunction. 2- Increased insudation of lipoprotein into the vessel wall. 3- A series of cellular interactions in these foci of injury involving ECs, T lymphocyte, SMCs of intimal or medial origin. 4- Proliferation of smooth muscle cells in the intima with formation of extracellular matrix by the SMCs.
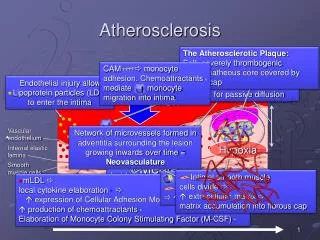
The response-to-injury of atherosclerosis #- illustration or response to injury of atherogenesis in these figure .
Those pictures considers AS a chronic inflammatory response of the vascular wall to a variety of initiating events that can occur early in life • Mechanisms contributes in plaque formation:- Endothelial dysfunction, Monocyte adhesion, Lipid and infarction, Smooth muscle proliferation, Extracellular matrix deposition, accumulation, Thrombosis
The response-to-injury of atherosclerosis 1-Endothelial injury:- Chronic or repeated endothelial injury is the cornerstone of the response to the injury hypothesis A- Homodynamic disturbances: - Disturbances perfusion to the tissue B- Advance effect of hypercholesterolemia, perhaps acting in concert
Hyperlipidemia contributes to atherogenesis in several ways:- * Chronic hyperlipidemia, particularly hypercholesterolemia, may itself initiate endothelial dysfunction. * Lipoproteins accumulate within the intima at sites of endothelial injury or dysfunction. * It provides the opportunity for modification of lipid in the arterial wall.
Oxidized LDL contributes to atherogenesis in the following ways:- * It is readily ingest by macrophages through the scavenger receptor that is distinct from the LDL receptor * It is chemo tactic for circulating monocyte * It increases monocyte adhesion
* It inhibits the motility of macrophages already in lesion. * It stimulates release of growth factors and cytokines. * It is cytotoxic to endothelial and SMCs. * It is immunogenic.
2- Complicated plaques * In advanced disease, plaques frequently undergo patchy or massive calcification, and arteries may be converted to virtual pipestems * Fissuring or ulceration of the luminal surface with rupture of the plaque may discharge debris into the blood stream (cholesterol emboli) * Fissuring or ulceration of the luminal surface with rupture of the plaque may discharge debris into the blood stream (cholesterol emboli)
* Fissured or ulcerated lesion may develop superimposed thrombosis * Hemorrhage into a plaque may result from loss of endothelial integrity (early ulceration), leading to progressive influx of blood from vessel lumen, or the hemorrhage may arise from the perplaque capillaries describe, and may lead to its rupture
Superimposed thrombosis Advanced atherosclerosis of the abdominal aorta
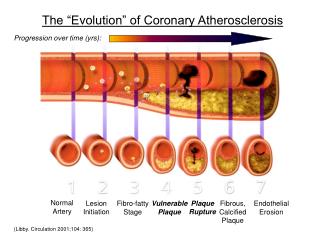
3- Rupture • Although the disease process tends to be slowly progressive over decades, it usually remains asymptomatic until an atheroma obstructs the blood stream in the artery • This is typically by rupture of an atheroma, clotting and fibrous organization of the clot within the lumen, coverage the rupture but also or over time and after repeated
4- Stenosis • Stenosis producing ruptures, resulting in a persistent • usually localized stenosis • It can be slowly progressive, while plaque rupture is a sudden event that occurs specifically in atheromas with thinner or weaker fibrous caps that have become "unstable”
Risk factors 1- Age: - Is a dominant influence, although early lesions of atherosclerosis appear in childhood 2-Sex: - Males are much more prone to atherosclerosis than females. Females are more or less sheltered from advanced disease-producing atherosclerosis until menopause, unless they are predispose by diabetes or hyperlipidemia or sever hypertension
Familial predisposition: - There is well-defined to AS and IHD. Acquired risk factors: - Diabetes, smoking hyperlipidemia, hypertension. Other factors: - Insufficient regular physical activity, obesity, high carbohydrate intake.
Signs and symptoms • Interfering with the coronary circulation supplying the heart or cerebral circulation supplying the brain causing stroke or heart attack. • Various heart diseases including congestive heart failure and most cardiovascular diseases. • Peripheral artery occlusive disease (PAOD).
Signs and symptoms related to cardiovascular disease 1- Chest pain(angina pectoris): - It is typically substernal radiating to the left shoulder, arm, or jaw 2- Subtle, progressive fatigue, weakness, and dyspnea (these symptoms usually appear on exertion) 3- Alteration in mental alertness, inability to concentrate, sleep disturbance
4- Myocardial infarction (MI): -The S&S of MI includes the following :- • Chest pain, unrelieved by rest or medication • Nausea and vomiting • Dyspnea • Orthopnea • Anxiety, severe apprehension • Denial • Dysrhythmias • Weakness
Diagnostic parameters: - 1- Laboratory findings:- A- Lipid profile :- Fasting lipid profiles, includes total cholesterol, LDL,HDL, and triglycerides B- Cardiac enzymes :- Creatine kinase (cK) C- Leukocytes count and sedimentation rate
2- Other diagnostic test A-ECG:- A 12- leads ECG is performed to determined if the patient with ASHD is having MI. B-Exercise stress test :- this is recording of an ECG during exercise . Coronary angiography (cardiac catheterization) :- catheterization of the R&L sides of the heart and the coronary arteries is performed to define suspected lesion of the coronary anatomy in terms of percentage of obstruction .
Treatment 1- thrombolytic 2- percutanous transluminal coronary angioplasty (PTCA) 3- intracoronary stent 4- Directional coronary atherectomy (DSA) 5- Coronary artery bypass grafting (CABG)
Nursing diagnosis 1- pain related to imbalance exist b/w oxygen supply and demand 2- Potential for decreased myocardial tissue perfusion related to imbalance exist b/w O2 supply and demand , as evidenced by dysrhythmias , or heart failure 3- Potential for anxiety related to the diagnosis of ASHD, treatment, and possibility of death