Download
1 / 22
220 likes | 243 Views
Learn about neurovascular assessment and imaging techniques for knee injuries, emphasizing vascular complications and peroneal nerve injuries. Key topics include vascular assessment, ankle-brachial index, selective angiography, and neurologic assessment methodologies.

E N D
Neurovascular Assessment and Imaging MehranSoleymanha(Ass. Prof. GUMS , Knee surgery fellowship, SBUMS, Akhtar Hospital) 24th Annual Meeting of the I.O.A– Tehran – Sep.29.2016
Vascular Assessment • Popliteal artery injury ………….. 32 % to 45% • Delayed recognition beyond 8 hours …………… amputation • The risk of vascular injury is independent of trauma intensity Alberty RE. et al. popliteal artery injury with fractural dislocation of the knee. Am J Surg 1981.
Vascular Assessment • Arterial injury can range from: • Transient kink • Intimal tear • Dissection • Acute thrombosis • Complete transection Tay AKL. et al. complications associated with treatment of multiple ligament injured. Knee Sport Med Arthrosc Rev 2011.
Vascular Assessment • Physical examination • Bilateral dorsal pedis- posterior tibial pulse • Capillary refill • Skin discoloration • Temperature change (5- 15 % False negative) McCutchan . et al. Injury to the popliteal artery associated with dislocation of the knee: palpable distal pulses do not negate the requirement for arteriography. Injury1989.
Vascular Assessment Ankle-Brachial Index (ABI) • The systolic blood pressure in the leg should be approximately the same as the systolic blood pressure in the arm. • The ratio of systolic blood pressure in the leg vs the arm should be approximately 1 or slightly higher. • ABI < 0.9 ……….. 87% sensitivity 97% specificity 91% P.P.V Adapted from Weitz JI, et al. Circulation. 1996;94:3026-3049.
Vascular Assessment Ankle-Brachial Index (ABI) Hiatt WR, N Engl J Med 2001;344:1608-1621
Vascular Assessment Ankle-Brachial Index (ABI) 100% negative predictive value ABI > 0.9 With Doppler probe Mills WJ , et al. The value of the ankle-brachial index for diagnosing arterial injury after knee dislocation: a prospective study. J Trauma. 2004
Vascular Assessment • Arterial / venous duplex • Non invasive • Less expensive • Limitation in obese patient • No specific study in knee dislocation Medina O, et al. vascular and nerve injury after knee dislocation: a systemic review. Clin Orthop Relate Res.2014 .
Vascular Assessment Selective angiography / CT angiography • Alternative to conventional angiography • Good sensitivity and specificity • Requires only antecubital venous cannulation • Less invasive • Costs effective • More time-efficient • 25% of radiation Gakhal MS, et al. CT Angiography signs of lower extremity vascular trauma. AJR 2009 .
Know or suspected knee dislocation or multiple ligament knee injury Reduce knee joint physical exam and ABI • Distal pulse absent • Active hemorrhage • Expanding pulsatile hematoma • Distal ischemia Distal pulse asymmetric or ABI <0.9 Distal pulse present and well perfused limb with ABI>0.9 Admit and observe for 24– 48 hr A/V Duplex 48 hr prior to surgical intervention To OR for surgical exploration Arteriogram / CTA Nicandri et al. Practical Management of Knee Dislocations: A Selective Angiography Protocol to Detect Limb-Threatening Vascular Injuries. Clin J Sport Med. 2009.
Neurologic Assessment • Proneal nerve injury ………….. 25% to 36% • Traction and stress varus mechanisms O’Malley et al. Treatment of Peroneal Nerve Injuries in the Multiligament Injured/Dislocated Knee. J Knee Surg. 2016.
Neurologic Assessment • Physical exam • Peroneal nerve / Tibial nerve Sensory / Motor function • EMG/NCV (3-4 week) • MRI • Edema • Hematoma • Mild contusion • Partial disruption • Perineural scar tissue • Neuroma • U.S • Nerve exploration O’Malley et al. Treatment of Peroneal Nerve Injuries in the Multiligament Injured/Dislocated Knee. J Knee Surg. 2016.
peroneal nerve injury Physical exam Complete nerve palsy Partial nerve palsy observe Consider Late Tendon Transfer O’Malley et al. Treatment of Peroneal Nerve Injuries in the Multiligament Injured/Dislocated Knee. J Knee Surg. 2016.
Complete nerve palsy - + Early operative intervention of ligament repair/ reconstruction Nerve exploration EMG/NCV testing at 3-4 weeks - motor action potential - US or MRI to assess nerve discontinuity observe + Repeat EMG/NCV at 3 &6 months Direct nerve repair and transfer (less than 3 months) neurolysis, grafting and tendon transfer based on intraoperative EMG/NCV Ho B et al. Treatment of Peroneal Nerve Injuries with simultaneous tendon transfer and nerve exploration. J Orthop Surg Res. 2014.
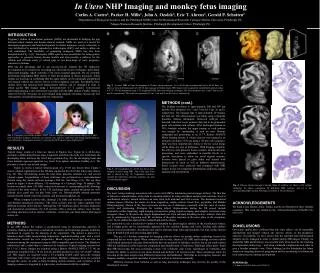
Area of extensive damage to the peroneal nerve Harvested sural nerve used to bridge injury zone just prior to cable grafting
Imaging • Radiography • Stress views • Intra operative fluoroscopic stress view • MRI • CT Scan
Imaging Standing bilateral AP Standing bilateral PA in 45 ̊ flexion • True lateral
Imaging Bilateral sunrise view • Alignment view
Imaging Stress view Varus stress radiograph Valgus stress radiograph > 2.7 mm LCL > 4 mm LCL & PCL > 4 mm MCL > 10mm MCL & PMC Difference Difference LaPrade RF. et al.The reproducibility and repeatability of varus stress radiographs in the assessment of isolated fibular collateral ligament and grade-III posterolateral knee injuries. An in vitro biomechanical study. JBJS.2008
Imaging CT scan
Imaging MRI