Download
1 / 94
980 likes | 1.39k Views
Neurovascular Disorders. CVA, TIA, Cerebrovascular defects, Head Injuries, Brain Tumors, Increased Intracranial Pressure, Epilepsy and Seizures. Objectives. Discuss various neurological disturbances in motor function and sensory/perceptual function

E N D
Neurovascular Disorders CVA, TIA, Cerebrovascular defects, Head Injuries, Brain Tumors, Increased Intracranial Pressure, Epilepsy and Seizures
Objectives • Discuss various neurological disturbances in motor function and sensory/perceptual function • Discuss the etiology/pathophysiology, clinical manifestations, assessment, diagnostic tests, medical management, and nursing interventions for a stroke patient
Objectives • List 5 signs of increased intracranial pressure and why they occur • List nursing interventions that decrease intracranial pressure • List 4 classifications of seizures, their characteristics, clinical signs, aura, and postictal period
Objectives • Discuss the etiology/pathophysiology, clinical manifestations, assessment, diagnostic tests, medical management, and nursing interventions for intracranial tumors, craniocerebral trauma, and spinal cord trauma
Objectives • Discuss patient teaching and home care planning for a patient with a neurological disorder
Stroke An abrupt impairment of brain function resulting in a set of neurologic signs and symptoms that are caused by impaired blood flow to the brain and last more than 24 hours
Risk Factors for Stroke Nonmodifiable factors Risk factors that cannot be changed Age, race, gender, and heredity Modifiable factors Those that can be eliminated or controlled Contributing causes: atherosclerosis, HTN, DM, obesity, smoking, high cholesterol, stress, cocaine use, sedentary lifestyle, oral contraceptives.
Vascular Problems • Stroke (cerebrovascular accident=CVA) • Also known as “brain attack” • Etiology/pathophysiology • Abnormal condition of the blood vessels of the brain, characterized by hemorrhage into the brain, or • Formation of an embolus or thrombus that occludes an artery ischemia to brain tissue affected by the occlusion
Figure 14-16 (From Lewis, S.M., Heitkemper, M.M., Dirksen, S.R. [2004]. Medical-surgical nursing: assessment and management of clinical problems. [6th ed.]. St. Louis: Mosby.) Three types of stroke.
Vascular Problems • Stroke cont. • Causes neurological deficits of sensation, movement, thought, memory, or speech. • Strokes may leave people with serious, long-term disability such as: • Hemiparesis • Inability to walk • Complete or partial dependence in ADLs • Aphasia or dysphagia
Vascular Problems • Clinical manifestations/assessment • Can affect body functions, personality, spatial-perceptual alterations, sensation and communication • The functions affected are directly related to the artery involved and the area of brain that it supplies. • Permanent damage can result due to anoxia of the brain
Strokes • Classified as : ischemic or hemorrhagic • Ischemic strokes are further classified as: • Thrombotic or embolic
Stroke: Pathophysiology Hemorrhagic stroke Blood vessel in brain ruptures; bleeding into the brain occurs Ischemic stroke Obstruction of blood vessel by atherosclerotic plaque, blood clot, or a combination of the two, or by other debris released into vessel that impedes blood flow to an area of the brain
Stroke • Thrombotic Stroke Thrombosis is the most common cause of stroke HTN and DM accelerate the atherosclerotic process • Seen most often in the 60-90 year old age group • If vessel becomes occluded ischemia infarction occurs • Usually occur in the larger vessels
Stroke • Thrombotic stroke cont. • Symptoms: tend to occur during sleep or shortly after rising • Neurological s/sx worsen for 72 hrs as edema increases in the infarcted area of the brain
Stroke • Embolic Stroke • The emboli most commonly originates from a thrombus in the endocardial (inside) layer of the heart • Caused by rheumatic heart disease, mitral stenosis, AF, MI, atrial-septal defects • Emboli travels upward to the cerebral circulation and lodges where a vessel narrows. • Most frequently occur in the midcerebral artery
Stroke • Hemorrhagic Stroke • Bleeding into the brain or subarachnoid space destroys or replaces brain tissue • Often caused by aneurysmswhich are a localized dilation of the wall of a blood vessel
Stroke • Hemorrhagic Stroke cont. • Aneurysm:usually caused by atherosclerosis, HTN, trauma, or infection, or congenital weakness in a blood vessel wall • It ruptures as a result of a small hole hemorrhage spreads rapidly. • Hemorrhage begins to absorb within 3 weeks • Recurrent rupture is a risk for 7-10 days after the initial hemorrhage
Transient Ischemic Attack Temporary neurologic deficit caused by impairment of cerebral blood flow Usually lasts less than 24 hrs.; most resolve within 3 hrs. Blood vessels occluded by spasms, fragments of plaque, or blood clots Important warning signs for the individual experiencing a full stroke
Transient Ischemic Attack Signs and symptoms Dizziness, momentary confusion, loss of speech, loss of balance, tinnitus, visual disturbances, ptosis, dysarthria, dysphagia, drooping mouth, weakness, and tingling or numbness on one side of the body; ataxia Between attacks, neurological status is normal
Transient Ischemic Attack • Medical diagnosis • Health history, physical examination findings, and results of brain imaging studies • CT without contrast media is the most important diagnostic study • Laboratory studies, electrocardiography (ECG), duplex ultrasonography, and cerebral angiography may also be used
Transient Ischemic Attack Medical treatment Depends on the location of the narrowed vessel and the degree of narrowing Acetylsalicylic acid (aspirin), ticlopidine hydrochloride (Ticlid), extended-release dipyridamole (Aggrenox), or clopidogrel bisulfate (Plavix) decrease platelet clumping Warfarin (Coumadin) and heparin - anticoagulants
Transient Ischemic Attack • Surgical Treatment may include: • Carotid endarterectomyand transluminal angioplasty • Carotid endarterectomy: removal of atheromatous lesion to enable increased blood flow • Transluminal angioplasty – the insertion of a balloon to open a stenosed artery to allow increased blood flow
Strokes • Assessment: • Subjective Data: description of onset of symptoms; presence of headache; sensory deficits: numbness, tingling, inability to think clearly, visual problems • Objective Data: presence of hemiparesis or hemiplegia; LOC, s/sx ICP, respiratory status, aphasia or dysphagia
Stroke • Diagnostic Tests • CT: can indicate size, location of the lesion and differentiate between ischemic and hemorrhagic stroke • MRI – can determine extent of brain injury • PET scan – useful in assessing the extent of tissue damage by showing the
Stroke • Medical management • If the patient has had a hemorrhagic stroke as a result of an aneurysm – surgery may be needed • Tie off or clip the aneursym; remove the clot • Treat [within 96 hrs. of bleeding] with calcium channel blockers x21 days
Stroke • Medical Management • Ischemic Stroke • Thrombolytics • T-PA (clot buster!) [Tissue Plasminogen Activator] Digests fibrin and fibrinogen lysing the clot; must be administered within 3 hrs of onset of symptoms • Pts. Screened carefully for coagulation disorders, recent GI bleed, r/o hemorrhagic stroke • May not be candidate for thrombolytic treatment • Patient choice factor
Stroke • Medical Management cont. • Ischemic Stroke cont. • Heparin and Coumadin – to prevent formation of more clots. Used after the first 24 hrs. if treated with t-PA • Drugs to reduce intracranial pressure: • Decadron (steroid) • Bowel meds (to reduce straining)
Stroke • Medical Management cont. • First 24-48hrs: • Airway maintenance and supportive treatment • Antihypertensives • Fluids restricted first few days • IV or Feeding tube may be utilized
Strokes • Medical Management cont. Other: • P.O. food/fluids: pureed, soft, regular • Neurological checks • Bedrest – depends on the type of stroke, deficits, and the judgment of the MD • Physical, occupational, and/or speech therapy
Stroke: Signs and Symptoms Different signs and symptoms, depending on the type, location, and extent of brain injury Hemorrhagic stroke Occurs suddenly; may include severe headache described as “the worst headache of my life” Other symptoms: stiff neck, loss of consciousness, vomiting, and seizures
Stroke: Signs and Symptoms Embolic stroke Appear without warning One or more of the following signs and symptoms: one-sided weakness, numbness, visual problems, confusion and memory lapses, headache, dysphagia, and language problems
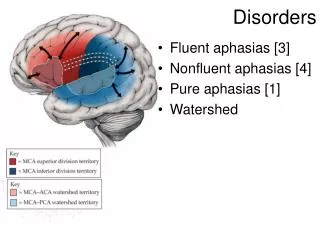
Stroke: Signs and Symptoms Aphasia A defect in the use of language; speech, reading, writing, or word comprehension Dysarthria The inability to speak clearly Dysphagia Swallowing difficulty Dyspraxia The partial inability to initiate coordinated voluntary motor acts Hemiplegia Defined as paralysis of one side of the body
Stroke: Signs and Symptoms Sensory impairment Unable to feel touch, pain, or temperature in affected body parts Unilateral neglect Do not recognize one side of the body as belonging to them Homonymous hemianopsia Perceptual problem: involves loss of one side of field of vision Elimination disturbances Neurogenic bladder Flaccid bladder Bowel incontinence
Prognosis Prognosis for TIA or stroke increasingly hopeful Critical variables for recovery: patient’s condition before the stroke, time between stroke and diagnosis, treatment and support in acute phase (usually the first 48 hours), severity of patient’s symptoms, and access to rehabilitative therapy Long-term recovery may depend on the care received immediately after the stroke Most recovery takes place in the first 3-6 months, but progress often continues long after that
Stroke • Nursing Intervention Goals during the initial phase are aimed at preventing neurological deficits • Neurological Assessments at regular intervals • Nutrition: route and texture depend on swallow ability • Self-care deficit and assistance needed. Start teaching process
Stroke • Nursing Interventions cont. • Elimination: insert/remove urinary catheter; monitor s/sx of UTI; bladder and bowel training • Mobility • ROM/exercise/activity: issue: unilateral neglect • Emotional lability/ depression
Stroke • Nursing Interventions cont. • Communication: many stroke patients have speech problems • ST will evaluate and treat • Approach in an unhurried way • Communication board may be helpful • Inability to articulate doesn’t mean cognitive impairment
Stroke • Patient Teaching • Techniques to compensate for the deficit(s) • “Rehabilitation” starts with admission to the acute facility • Medication instruction • “Stroke Club” referral for support • Safety • Communication • Caregiver stress relief
Nursing Care in the Rehabilitation Phase Interventions Self-Care Deficit Risk for Injury Ineffective Coping Impaired Verbal Communication Imbalanced Nutrition Impaired Physical Mobility Constipation Total and Functional Urinary Incontinence
Discharge Patients may be discharged to home or go to specialized rehabilitation centers for continued therapy Outpatient therapy is an option for some patients When able, patients are transitioned back into the home setting Essential to include family, friends, and significant others in this process