Download
1 / 39
390 likes | 532 Views
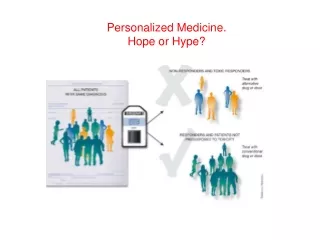
Drug design, from hype to Hope forever. And what does 3DM have to do with that?. Life expectancy. World life expectancy goes up because of hygiene, medication, mechanical improvements, and knowledge. Sub S ahara Africa went down over Aids.

E N D
Drug design, from hype to Hope forever And what does 3DM have to do with that?
Life expectancy World life expectancy goes up because of hygiene, medication, mechanical improvements, and knowledge. Sub Sahara Africa went down over Aids. Cancer is now the #1 killer in The Netherlands because mechanical improvements (surgeons avoiding that people die from hearth attacks). Money matters.
Medicine is from all times The Edwin Smith Papyrus documents ancient Egyptian medicine, including the diagnosis and treatment of injuries.
Aspirin Plant extracts, including willow bark and spiraea, of which salicylic acid was the active ingredient, had been known to help alleviate headaches, pains, and fevers since antiquity. The father of modern medicine, Hippocrates, who lived sometime between 460 BC and 377 BC, left historical records describing the use of powder made from the bark and leaves of the willow tree to help these symptoms. Aspirin was first isolated by Felix Hoffmann, a chemist with the German company Bayer in 1897. In 1971, British pharmacologist John Robert Vane, then employed by the Royal College of Surgeons in London, showed aspirin suppressed the production of prostaglandins and thromboxanes. For this discovery he was awarded the 1982 Nobel Prize in Physiology or Medicine, jointly with Sune K. Bergström and Bengt I. Samuelsson. So far for rational drug design…
But, medicines do help In 1900, one-third of all deaths in the U.S. were from three general causes that are rare today because they are preventable and/or treatable: pneumonia, tuberculosis, and diarrhoea. By 1940, the chance of dying from these three causes was 1 in 11; by 2000, the odds were down to 1 in 25. In 2002, the ‘innovation gap’, or cost of the learning curve expressed in the difference between the money spent and the number of new drugs approved, was the largest it has been in 15 years for the industry as a whole. Just last year, pharma spent $32 billion in R&D, but received approvals on only 25 new drugs. The $32 billion was double what the industry spent on R&D in 1997, and three times the sum spent in 1992.
Money matters From 1950 to 2008, the US Food and Drug Administration (FDA) approved 1,222 new drugs (new molecular entities (NMEs) or new biologics). However, although the level of investment in pharmaceutical research and development (R&D) has increased dramatically during this period — to US$50 billion per year at present — the number of new drugs that are approved annually is no greater now than it was 50 years ago. Indeed, in 2008, only 21 new drugs were approved for marketing in the United States, which is well below the level required to secure the future of the pharmaceutical industry (Munos, ref 7)
Desperate people do desperate things Moerman: De Nederlandse huisarts Cornelis Moerman (1893 - 1988) bedacht een nogal spartaans dieet gebaseerd op het (onjuiste) idee dat duiven en Franse wijnboeren geen kanker krijgen, en dat dus duivenvoer kanker geneest. Het dieet is wegens de grote populariteit meerdere malen onderzocht, en samenvattend kan men zeggen dat het aantal genezingen na een moermandieet iets lager is dan het normale en uiterst kleine aantal spontane genezingen van kanker.
Desperate industries do desperate things There are multiple reasons for the pattern of high-roller sales followed by dry-spells. One that has received much attention has been the dependence on large blockbusters. When a company like Pfizer has $12.9 billion in revenues coming from Lipitor alone, a tremendous hole occurs when the patent for that medicine expires, as Pfizer has recently experienced. In looking at projections, Merck might be in the same boat by 2018 as Januvia sales will be almost 25% of Merck’s total revenues. And whenever income goes down, they start buying into hypes.
The first hype Hol (ref 13) coined the name ‘rational drug design’ for all protein-structure based techniques, thereby implicitly calling all methods that actually worked, such as screening or luck, irrational. Methotrexate in the active site pocket of dihydrofolatereductase . Hol wrote: “As to whether a drug can actually reach its target, e.g. the active center of an enzyme, is primarily a spatial problem. Assuming that the structures of both components are known, computer graphics can help in checking the suitability of a potentially active substance. As example, the structure of the complex formed between a bacterial dihydrofolate-reductase, NADP and the anticancer drug methotrexate is shown on the right. As one can see, it fits”
Another hype A hype that lasted >25 years is that bigger computers will solve everything (they share this hype with MD people). First to calculate small molecule structures with QC, QM, etc. But this precision was never needed because the targets normally were poor homology models. Ligand conformations in vacuo often have little to do with the bound situation. Then for docking (first without flexibility). Then for CoMFA (something like inverted SAR…). Then for virtual screening.
Other hypes A hype that lasted >25 years is that bigger computers will solve everything (they share this hype with MD people). First to calculate small molecule structures with QC, QM, etc. But this precision was never needed because the targets normally were poor homology models. Ligand conformations in vacuo often have little to do with the bound situation. Then for docking (first without flexibility). Then for CoMFA (something like inverted SAR…). With variants like Ludi. Then for virtual screening.
Other hypes A hype that lasted >25 years is that bigger computers will solve everything (they share this hype with MD people). First to calculate small molecule structures with QC, QM, etc. But this precision was never needed because the targets normally were poor homology models. Ligand conformations in vacuo often have little to do with the bound situation. Then for docking (first without flexibility). Then for CoMFA (something like inverted SAR…). With variants like Ludi. Then for virtual screening.
Recent hypes The new hype is ‘translational science’. Wikipedia: “In the field of medicine, for example, it is used to translate the findings in basic research more quickly and efficiently into medical practice and, thus, meaningful health outcomes, whether those are physical, mental, or social outcomes”. The translation science hype is feeling stiff competition from systems biology and modelling pharmacokinetics and pharmacodynamics. Between the lines we read in translational science that the pharmaceutical industry has finally realized that our deep lack of understanding of all aspects of the interaction of a medicine with a human being is the main cause for luck still being the most determining factor in the drug design process. Consequently, we see the out-sourcing budgets of the large pharmaceutical industries go up, and more and more fundamental research performed in academia is finding its way to small and medium size enterprises (SMEs) where it can be incorporated in their lean and mean research machines.
A 20 year hype But, Bas did ‘win’ the GPCR-DOCK competition.
But where do we fail? blood–brain barrier
But where do we fail? cytochrome P450
But where do we fail? Thermodynamics
But where do we fail? ADME-tox
Serendip http://en.wikipedia.org/wiki/The_Three_Princes_of_Serendip Correlation analysis; text mining (RDF); Visualistion; you.