Download
1 / 15
170 likes | 438 Views
The Iliopsoas Muscle. Accession 112303. Anatomy of the Iliopsoas (Miller). Fusion of the psoas major and iliacus muscle Ventral to the quadratus lumborum and dorsal to the psoas minor, which it covers laterally

E N D
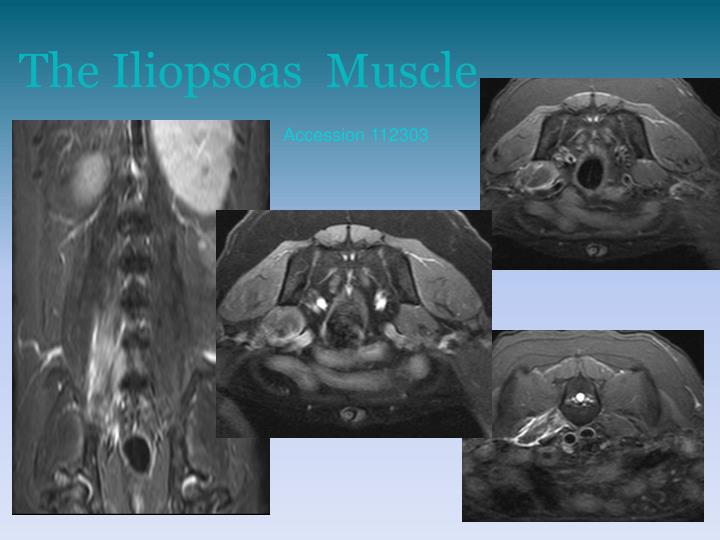
The Iliopsoas Muscle Accession112303
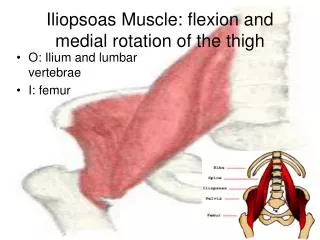
Anatomy of the Iliopsoas (Miller) • Fusion of the psoas major and iliacus muscle • Ventral to the quadratus lumborum and dorsal to the psoas minor, which it covers laterally • Psoas major-Arises from the transverse processes of L2 and L3, attaches via ventral aponeurosis of quadratus lumborum to L3, L4 and on the ventral and lateral surfaces of L4-7 • Iliacus arises from the smooth ventral surface of the ilium and joins psoas major • Together they insert lesser trochanter of the femur
Action and Innervation (Miller) • Draw the pelvic limb forward through flexion of the hip joint • When the femur is fixed in position, will result in flexion and fixation of the vertebral column • When leg is extended backward, will draw the trunk backward • Innervated by the rami ventrales of the lumbar nerves
Muscle strains (Slatter) • Injury results in tearing of muscle fibers, pain, spasm of the injured area, muscle fascia, and hemorrhage. Grading schemes exist based on the amount of muscle and fascial tearing and the amount of hemorrhage • Chronic injury results in atrophy and fibrosis • Most common site is at the musculotendinous unit
Iliopsoas strains (Slatter) • Iliopsoas and tensor fascia latae muscle strains may be confused with hip dysplasia, with pain on hip extension • Internal rotation and hip extension elicits more excruciating signs than hip dysplasia alone • Mostly treated conservatively, more severe grades may benefit from surgical debridement and closure if apposition can be maintained
Traumatic injury of the iliopsoas in 3 dogs • History: lameness after playing, being caught in the fence, injury by pellet gun • PE findings: pain on hyperextension or abduction of the hip joint, extension and internal rotation had decreased RO, deep palpation of the lesser trochanter marked pain , shortened forward stride, muscle atrophy of pelvic limb in chronicity • US findings: hypoechoic and swollen acutely. Chronically hyperechoic focus • Two responded to rest/NSAIDS, the third had numerous recurrences and had a tenomyectomy and resolved clinical signs
US of the normal iliopsoas muscle • Psoas major-identified ventral to the vertebral bodies of L4-7: hypoechoic muscle with longitudinal linear hyperechogenicities interspersed • Iliacus muscle: origin difficult to visualize as separate from the psoas major • Insertion: medial thigh, trace the femur proximal toward the coxofemoral (CXF) joint until lesser trochanter identified: small focal protrusion from the medial surface of the femur, several cm distal to CXF joint • Myotendinous junction easily visualized; tendon is short, hyperechoic, and linear
US of the normal iliopsoas muscle • Expected changes with trauma: enlargement with hypoechoic regions likely representing edema, inflammation, and hemorrhage in acute stages • Changes expected with chronic trauma: hyperechoic areas likely fibrosis or ectopic mineralization • CT and MR imaging may be more sensitive than ultrasound in humans for iliopsoas injury
CT features of suspected trauma • Asymmetric enlargement of the iliopsoas • Multifocal hypoattenuating regions within the musculature (edema and inflammation?) • Nonuniform contrast enhancement of iliopsoas, tensor fasciae latae, and sartorius • Mild, acute injuries may not be identified on CT • Concurrent femoral neuropathy-compression from iliopsoas?
Traumatic avulsion fracture of the lesser trochanter STIR TIW + C
Traumatic avulsion fracture of the lesser trochanter • Humans-avulsion fractures of the lesser trochanter, most commonly seen in male adolescent athletes 13-17 yo • Adults are more likely to rupture muscle than fracture (an abstract said dogs with iliopsoas have a average age 4.1 yrs)
Femoral neuropathy with iliopsoas muscle injury • Femoral neuropathy associated with iliopsoas muscle pathology is well-described in humans • Assoc with hematoma formation with bleeding disorders • Femoral neuropathy; mild decrease in patellar reflex, extreme lameness, focal denervation of the distal quadriceps femoris • Atrophy of the right iliopsoas muscle, increase signal on T2W, non-contrast enhancing • Ddx for hyperintensity: inflammatory infiltrate, edema, or chronic hemorrhage • Biopsies and tenectomy performed: atrophy, degeneration, occasional necrosis; no evidence of inflammation, hemorrhage, or neoplasia • Fibers were partially replaced with fat; cause for signal change?
References • Breur G, Blevins W. Traumatic injury of the canine iliopsoas muscle. J Am Vet Med Assoc 1997;210:1631–1634. • Cannon MS, Puchalski SM. Ultrasonographic evaluation of normal canine iliopsoas muscle. Veterinary radiology & ultrasound, vol. 49, no. 4, 2008, pp 378–382. • Rossmeisl JH, et al. Computed tomographic features of suspected traumatic injury to the iliopsoas and pelvic limbmusculature of a dog. Veterinary Radiology & Ultrasound, Vol. 45, No. 5, 2004, pp 388–392. • Vidoni B, et al. Traumatic avulsion fracture of the lesser trochanter in a dog. Vet Comp OrthopTraumatol 2005; 18: 105–9. • Stepnik, MW, et al. Femoral Neuropathy in a Dog with Iliopsoas Muscle Injury. Veterinary Surgery 35:186–190, 2006. • Montgomery G, Fitch R. Muscle and Tendon Disorders. In Slatter (ed): Textbook of Small Animal Surgery. 3rd edition. Saunders, Philadelphia, 2003, p 2264-2271. • Evans HE. Miller’s Anatomy of the Dog. 3rd edition. WB Saunders, Philadelphia, 1993, p 349-355.