Download
1 / 43
470 likes | 896 Views
Anaerobic Bacteria. Fundamentals II Stephen A. Moser, Ph.D. 10/19/2011. Categories Based Upon Gaseous Requirements. Aerobic bacteria Require oxygen as electron acceptor Microaerophilic bacteria Require oxygen in reduced quantity Capnophilic bacteria Require carbon dioxide

E N D
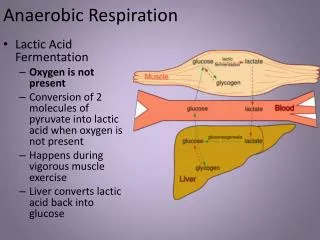
Anaerobic Bacteria Fundamentals II Stephen A. Moser, Ph.D. 10/19/2011
Categories Based Upon Gaseous Requirements • Aerobic bacteria • Require oxygen as electron acceptor • Microaerophilic bacteria • Require oxygen in reduced quantity • Capnophilic bacteria • Require carbon dioxide • Facultative bacteria • Grow either with or without oxygen • Anaerobic bacteria • Both obligate and aerotolerant
Physiology And Growth Conditions • Both pH and oxidation-reduction potential are important. • Cytochrome systems absent. • Most lack superoxide dismutase (SOD) and catalase. • Obligate anaerobe - lack cytochrome, SOD and catalase. • Aerotolerant anaerobe - has some SOD and or catalase. • Facultative anaerobe - grow equally well under either aerobic or anaerobic conditions.
Anaerobic Bacteria in Ocular Infections • Conjunctivitis • Keratitis • Dacryocystitis Brook I. Anaerobic and aerobic bacterial flora of acute conjunctivitis in children. Arch Ophthalmol 1980; 98: 833–835.
Anaerobic InfectionsGram-negative Bacilli • Bacteroides / Prevotella / Porphyromonas species • Non-spore forming, pleomorphic rods • Normal flora of upper respiratory tract, intestinal and female genital tract • Most important groups - Bacteroidesfragilis and Prevotellamelaninogenica • Colon associated –group (fragilis) • Upper respiratory tract - P. melaninogica group • Female genital tract - P. bivia and P. disiens • Clinical disease usually abscess formation with mixed anaerobic and facultative anaerobic bacteria.
Anaerobic InfectionsGram-negative Bacilli • Fusobacterium • Pleomorphic non-spore forming rods • Usually present in mixed infections but may be the sole agent • Present in both upper respiratory and intestinal tract • F. necrophorum – Lemierre’s syndrome • Jugular vein thrombosis
Anaerobic InfectionsGram-positive Bacilli • Actinomyces • Most common is Actinomyces israelii • Slow growing and are difficult to isolate • Cause extensive soft tissue involvement crossing tissue plane and involving multiple organ systems • Can result in draining sinus tracts with “sulfur granules” • Associated with oral, respiratory and female genital tract infections (IUD)
Actinomycosis “Lumpy Jaw”
Anaerobic InfectionsGram-positive Bacilli • Propionibacterium • Unusual cause of infection • Normal flora of the skin • May be difficult to determine the role of blood isolates in disease • Lactobacillus • Normal flora of the vagina • Rare cause of disease • Eubacterium, Bifidobacterium, Arachnia
Anaerobic InfectionsSpore forming Gram positive Bacilli • Clostridium • The only genus of anaerobes that forms spores • Tetanus - C. tetani - in vivo toxin production • Tetanospasmin – blocks inhibitory neurotransmitters • Botulism - C. botulinum - ingestion of preformed neurotoxin except for wound and infant botulism • Blocks release of acetylcholine • Gas gangrene - C. perfringens - H2 & CO2 • Phospholipase C (-toxin) • Food poisoning - C. perfringens • Enterotoxin • C. septicum - associated with malignancy, neutropenia • Pseudomembranous colitis / antibiotic associated diarrhea - C. difficile
Clostridiumperfringens Nagler Test
Pathogenesis • Synergy with facultative organisms. • Facultative bacteria such as Enterobacteriaceae function to reduce the oxygen content in the tissue. • Beta-lactamase production. • Capsule of Bacteroidesfragilis is antiphagocytic. • Toxin production.
DIAGNOSIS OF ANAEROBIC INFECTIONS • Clinical signs • Foul smelling discharge • Proximity to a mucosal surface • Gas in tissue • Abscess formation • Gram stain • May be helpful in the establishment of a mixed infection or the presence clostridia in wounds
DIAGNOSIS OF ANAEROBIC INFECTIONS • Culture • Sample collection and transport are critical • Require complex medium supplemented with hemin, Vit. K and or blood. • Should include media containing antibiotics (aminoglycoside) to suppress facultative anaerobes, e.g., E. coli • Incubation and work up performed in CO2 in nitrogen/ hydrogen mix
Treatment Of Anaerobic Infections • Surgical drainage of closed abscess. • Mixed infections - cover for both aerobic and anaerobic component. • Metronidazole, penicillin G, Clindamycin. • Penicillin resistance is common among some species, e.G. P. melaninogenica group, B. fragilis groups. • Aminoglycosides not effective. • Toxin mediated diseases - antitoxin and antibiotics if active infection vs. Intoxication.
Objectives • Know the different gaseous requirements of bacteria. • Know what special collection and diagnostics methods are required to isolate anaerobes. • Know the epidemiology of anaerobic infections. • Recognize the clinical syndromes associated with anaerobic bacteria.