Download
1 / 8
80 likes | 93 Views
Urinalysis CPC (Renal block) Thursday Sep 5, 10-12am. Activities for this 2-hour session: Review Urinalysis CPC Student Handout , including the following information: CPC session explanation of activities General Urinalysis laboratory procedure Practice Questions (optional)

E N D
Urinalysis CPC (Renal block) Thursday Sep 5, 10-12am Activities for this 2-hour session: • Review Urinalysis CPC Student Handout , including the following information: • CPC session explanation of activities • General Urinalysis laboratory procedure • Practice Questions (optional) • Review You-Tube Videos • Review Microscopic Image file • Review Urinalysis CPC Cases for Interpretation (9 total) • 10-question quiz at 11:30 am
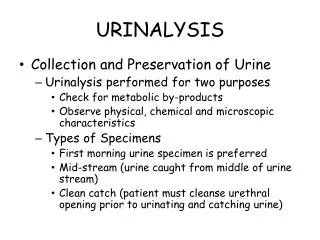
URINALYSIS AND URINE CULTURE View the following videos on YouTube: • “Clean Catch Urine”, 4:19 – This video explains how to obtain clean-catch urine samples on both male and female patients. • “no intro Urinalysis”, 1:19 – This video explains how to use the urinalysis dipstick. C. “urine cultures”, 4:39 – This video gives an overview of urine cultures.
Macroscopic analysis Chemical analysis Microscopic analysis
Nephrotic Syndrome • Clinical syndrome: 1. Massive proteinuria ( > 3.5 gr/day in adult) 2. Hypoalbuminemia (plasma albumin < 3 gm/dL) 3. Generalized edema • Hyperlipidemia and lipiduria • Usually no azotemia, hematuria or hypertension at onset • Can see fatty casts and oval fat bodies in urine microscopically
Causes of Nephrotic syndrome (Robbins 9th ed, Table 20-7, page 915)
Nephritic Syndrome • Clinical syndrome with acute onset: • hematuria (typically with dysmorphic RBCs and RBC casts) • oliguria and azotemia • mild to moderate hypertension • May see proteinuria and edema, but not usually severe • Unifying histologic picture of cellular proliferation in glomeruli, usually with leukocytic infiltration(hypercellularity) • Inflammation injures capillary walls, leading to loss of RBCs into urine & RBC cast formation • Hemodynamic changes lead to reduced GFR oliguria, azotemia, and some fluid retention • Hypertension probably due to fluid retention and likely renin release due to decreased perfusion to glomeruli (ischemia) • Can be due to primary glomerular disease or secondary to a systemic disorder • Examples: Post-streptococcal (post-infectious) GN & Crescentic GN; see also Lupus GN (later)