Download
1 / 53
530 likes | 587 Views
Understand levels of adult responsiveness to a child's emotional regulation, from proactive growth factors to reactive strategies. Learn effective communication, recognition of distress, and strategies for all-day communication and behavior management.

E N D
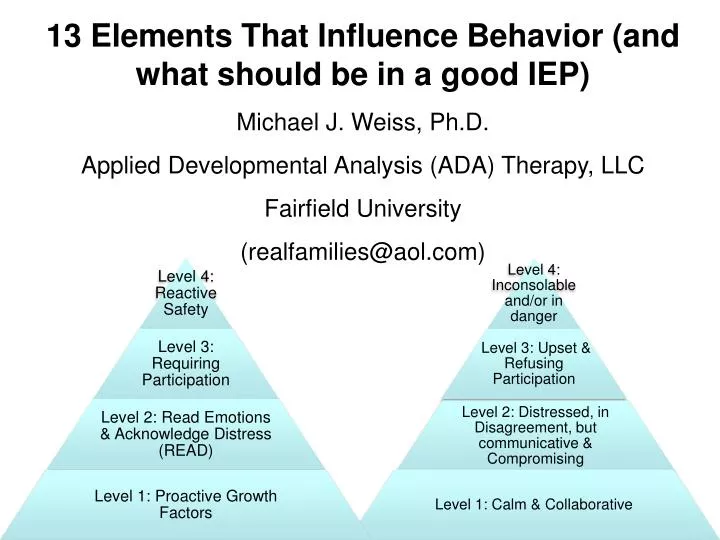
13 Elements That Influence Behavior (and what should be in a good IEP) Michael J. Weiss, Ph.D. Applied Developmental Analysis (ADA) Therapy, LLC Fairfield University (realfamilies@aol.com)
A Developmental system for thinking about self-regulation and adult supports
Four levels of adult responsiveness to child’s levels of emotional regulation • Level 1: Proactive growth factors • Need for meaningful education, therapy & relationships • Need to "push the envelop of growth" in emotional regulation • Level 2: Read Emotions & Acknowledge Distress (READ) • Need for recognition, acknowledgement and communication related to a person's distress, disagreement or other forms of refusal • Need to return to proactive growth factors through communication, collaboration & compromise • Level 3: Adult insistence on participation • Interaction partners need to both recognize the difference between a request/choice and a "requirement” • If the activity is a "requirement” – adult must “compel” participation • Need to move past point of conflict and through the activity • Level 4: Reactive strategies to extreme distress & actions • Need to keep everyone safe • Need to create calm & return to proactive growth factors
Level 1: proactive factors & strategies that influence children’s growth & behavior • Definitions & Data • Medical team evaluation • Relationships and finding my child’s (and my) voice • Communication • Sensory & movement issues • Multimodal channels of information • Intensity, diversity, generalization • Assume competence: offering a wide academic window • Inclusion in the world • Make plans do-able • Understand your belief-systems • Dynamic behavior (“parenting”) plan • Medical management
Level 1.1: Definitions & data: be evidence based • Have you defined the behaviors, educational and therapeutic targets of concern? • Factually note: what, where, when, who • What happened before and after events • Indicate “antecedents” and “consequences” or environmental factors • Record frequency and duration of events?
But, beware of “data-ists” • You know… racist, sexist, dataist…. • The “big data lie” – “there is no data…” • Beware of statements like, “the literature indicates…” • “no data” is interpreted to mean “no truth” • Concerning most therapies, what should be said is that “it hasn’t been appropriately studied yet” • Assessing issues in clinical settings is time consuming, costly, hard-to-control & contrary to providing services “right now” • That doesn’t mean intuition should be ignored • Nor, does it mean that we should NOT collect information “An absence of evidence is not evidence of absence (Dr. Carl Sagan) ”
Level 1.2: Medical team evaluations Pervasiveness of medical issues that follow our kids, i.e., Neurological, Gastrointestinal anomalies • See Tim Buie in Bauman & Kemper (2004) Neurobiology of Autism • Who is the total team that is sharing information • Neurologist, Geneticist, Endocrinologist, ENT, Urologist, Immunologist, Orthopedist, GI, Dentist, & more…. • Psychopharmocology generally, put in place non-medical interventions of behavioral development first – use of medications should routinely “go last”
Level 1.3: Recognizing the PERSON: Finding your child’s “voice” • What does your child like to do? What do they gravitate toward? • Consider the who, what, where, when of actions in terms of “why” • go beyond the facts and make guesses about motives and desires about what is motivating a child’s behavior • Yet, recognize the fallibility of guessing! • Enlist your child on his/her terms • Join in (Floor time/Relationship Development Intervention) • Offer age-appropriate options, choices & autonomy • Create therapeutic opportunities for self-expression • Have you asked the child/student/patient “why” they do what they do or how they feel about what is going on?
Level 1.4: Communication • Communication occurs ALL DAY • Not “two times 30-minutes” • Should NOT require a Speech & Language Pathologist • Training staff & family is the life blood of all-day communication • Total Communication systems • Verbal behavior programs • Gestures & Sign • Picture-symbol-systems • Augmentative and Alternative Communication (AAC) • Schedules, aided Language boards & use of “visuals” • MUSIC • Teaching THE ALPHABET!! • Have you given the child a means of saying what they might like to say? • “None of the above” • “More string to ‘stim’ with please” • “Drop dead you jack-ass”
Level 1.4: Communication Using music & reading to access speech & language
Level 1.4: Communication • Discussions of feelings, thoughts, desires • Social-affective-emotional vocabulary • Social curricula with instruction in pragmatics • “Social grammar:” turn-taking, reading cues, etc. • Learn how to anticipate what others’ are saying • Learn how to interpret others’ feelings about what they are saying • Use commercially available curricula as instructional/therapeutic guide • Age-typical partners: don’t let your child’s only communication partners be adults and other children with developmental concerns • Rehearsal of social communication • Social stories • Social scripts • Video models and video self-monitoring
Social script rehearsal for “Maine” conversations Pam: Do you ever go skiing in the mountains? Megan: Yes, I go skiing in the mountains. Pam: What else can you do in the mountains? Megan: I can go sledding. I can go hiking up a mountain path. Pam: What else? Megan: I can climb rocks. Pam: What do mountains look like? Megan: Mountains are tall. Mountain peaks are pointed. Sometimes snow is on the mountain peak, even in the summer. Pam: When there is a lot of snow in the driveway what do you need to do? Megan: I need to shovel the snow to clear the way.
Level 1.5: Sensory & Movement realities • Recognizing autism (and a wide host of other developmental disorders) as a “sensory-movement disorder” • Consider what types of therapies influence movement regulation in others’ that share the diagnosis of ASD • Consider other forms of movement disorders (i.e., issues related to cerebellum or basal ganglia; Parkinson’s; stroke patients, etc.) and what therapies help these individuals
The Neurobiology of Movement Disorders & Autism (Bauman, 2008; Bauman & Kemper, 2005; Courchesne & Allen, 1997; Hollander, et al., 2005) • The embryological early anomalies to effect development: • Brainstem/Inferior Olive • Cranial nerve development • Somatosensory information • Cerebellum • Regulates all movement • Regulates sensory processes • Motor, language & cognitive planning, sequencing, timing & organization • Basal Ganglia • Enlarged aspects (right caudate/total putamen volume) correlates with uncontrolled or perseverative movement
Autism is a movement disorder! • Correlations among aberrant movement patterns in: • Speech • Ballistic/Aberrant & repetitive movements • Throwing • Grasp/hand use • Lip Closure • Gait • Hopping & jumping • Reaching/Crossing midline • Kneeling & standing What might they have in common? • Disassociation of movement of different body parts • Difficulties in core strength, idiosyncratic weakness and/or hypotonia • Balance and coordination dysregulation • Cerebellum and Basal Ganglia regulation?
Level 1.5: Sensory & Movement realities • Recognizing environmental “contributions” (“noise” in any sensory modality) • Again, therapies are ALL DAY • “Sensory Diets”: managing arousal cycles • Oral-motor programming and daily carry-over • Real movement opportunities • Movement/expressive therapies (music/dance/art) • Break-a-sweat exercise • Use “incidental” exercise: sitting on a stool • Organize when movement is and is not encouraged
Level 1.6 Considering multimodal channels of information • Which modalities of taking in information goes with the least distress (seeing, hearing, touching??) • How to systematically combine modalities: • Play with modalities one at a time • Systematically add, subtract, mix modalities • Use behavior as an index of too many or too few? • Most common “good combination?” • Use visual information more • Talk at children less • Incorporation of touch that suits the child
Level 1.7: Understanding Intensity, diversity & generalization strategies • Intensity means: • hundreds of repetitions daily to further responsiveness • long periods of time dedicated • “early intervention” for 3-hours/week exemplifies “non-intensity” • Diversity of experiences effects attention • Moderate novelty in activities associated with alerting • Redundancy is associated with inattention (i.e., habituation) • Teach with intensity and diversity promotes generalization – systematically put in long hours with several differing: • Ways of presenting materials • People • Locations • Orders of activities • Repetition of activities through the day (rather than all at once)
Intensity-diversity-generalization of exposure to curricula • Communication systems are an all day requirement • Assistive technologies are omnipresent (verbal behavior; aided language boards; software; communication devices; picture-symbol systems) • Expansion into the “personal world” of interest-reality themes • Expansion into the social world (social scripts; social stories; functionality in the real world) • Table-top activities in support of real-world activities (how instruction traverses different methodologies) • Taught through diverse medium/methods (i.e., learning to read music) • Taught in a generalized manner; learned for generalize application
Level 1.8: Assuming competence: offering the dignity of age-appropriate curricula • The “retardation” or the “not ready yet” assumptions • Performance is a measure of competence? Ask a person diagnosed with Cerebral Palsy if they agree • Work at the child’s “developmental level?” Which is….? Fallacy of IQ or Developmental Quotients as global indicators • Discussions that the child can hear (but, shouldn’t) “stick of furniture” phenomenon • Assuming high level of performance is a “splinter skill” or an “odd” behavior is the death of developing person-specific abilities/skills
Level 1.8: Assuming competence: offering the dignity of age-appropriate interactions and curricula So…what should be our guide? • Have a great teacher as one of our guides! • Do use a tracking device (i.e., Activities of Basic Learning & Language Scales (ABLLS)) or other measurable data systems • Avoid “linear programming” and “mastery criteria” as only mechanism of change • Select a developmentally “wide window” of activities concurrently • Vary extent of supports v. level of independence as a function of task complexity, i.e., high-level activity with “errorless” supports • Select activities that lend themselves to age appropriate modifications • What is an age-appropriate version of the child’s obsessions or preoccupations?
Simple Sentence Structure EER: Plurals EER: Prepositions First Categories Adjectives & Opposites Words & Concepts I, II & III Concentrate! I Follow Directions: 1 & 2 Level Commands Micro-LADS programs (i.e., Prepositions & Pronouns) Sentence Master 1, 2, & 3 Number Maze Dollars and Cents Picture Sentence Key 1 Picture Sentence Key 2 Pix Writer Clicker 5 First Keys to Literacy All My Words Write: Out Loud Simon Sounds It Out 2 Visual Voice Typing Quick and Easy Black Beauty Level 1.8: Assuming competence: offering the dignity of age-appropriate curriculaAcademic computer software offering a “wide window” of intellectual opportunity (without the “social distractions”)
Software companies that you should know about • Don Johnston • Laureate Learning Systems • Crick Software
Level 1.9: “Inclusion” in the world • Real relationships: friends, loved ones and being a legitimate member of our community • Modeling and “regression toward the mean” • Organizing and generalizing our day-to-day conduct – don’t avoid going out • Catch-22 irony: why aren’t our kids included? Usually related to complicated behavior. Why is behavior complicated? Partly because we aren’t included in the world. • Going out IS HARD TO DO! • Promoting behavior in the world? Don’t want to “make a scene”
Level 1.10: Make plans Do-able • Figuring out how much you can realistically do • “Prep time” for all involved • REAL training and consultation of teaching staff and family (not “15-minutes per week consult”) • Team meeting opportunities • Formalizing fun time together • Formalizing fun time apart • Getting a babysitter • In-home services • Insistence on sufficient staffing
Connecticut “Bill 301” – Family Insurance coverage for ASD’s • Coverage for behavior services, OT, PT, Speech/Language (home programs) • Must be a diagnosis of ASD’s • Age and amount ($) of coverage • 2 to 9: $50,000/year • 9 to 13: $35,000/year • 13 to 15: $25,000/year
Level 1.11: Beliefs about childrearing and my child • Wanting change is not mutually exclusive with accepting people for who they are • People diagnosed with a developmental difference are still children, adolescents, adults • Interact with each individual according to both developmental status and chronological age • Yet, at no point across development is harming yourself or others acceptable behavior • Beliefs about competence translates into levels of expectations • Expectations establish comfort zone for what we will insist of our children • Young man in Westport, CT diagnosed with Asperger’s who drives himself to University • “I (teacher/parent/therapist) am entitled to respect and deference from my child/student/client, just as I owe them respect and deference”
Level 1.12: A flexible & dynamic behavior (“parenting”) plan • Predicated on concepts from the study of social development (i.e., children benefit from “authoritative” parenting), not from animal models of learning • Children do well in a climate combining unconditional love & support, with high standards & expectations • Understanding basic principals of Operant Theory is extremely useful in understanding how you are parenting/teaching a child • Know the definition of (i) positive reinforcement; (ii) negative reinforcement; (iii) punishment; & (iv) extinction • Principal focus of contingencies should revolve around “self-determination” (or the restrictions there of) • “Naturally occurring” consequences of doing what you want if you are comporting yourself appropriately… or not.
Level 1.13: Data-driven medical management • Going in “the right order”: points 1 through 12 above go first whenever possible • Obvious medical exceptions i.e., seizure activity, medical illness, disease, conditions, etc. (see point #2)) • Find a physician who: (i) you like!; (ii) returns your phone calls; (iii) is data driven; (iv) who asks about the educational/therapeutic programs; (v) is willing to try a diverse set of approaches • Back to point #1: define what you are doing and collect data • Be able to define what you are treating • If medical treatment isn’t working… CHANGE OR STOP!! • Identify “blind evaluators” in the data collection process
Level 1: proactive factors & strategies that influence PEACE • Definitions & Data • Medical team evaluation • Relationships and finding my child’s (and my) voice • Communication • Sensory & movement issues • Multimodal channels of information • Intensity, diversity, generalization • Assume competence: offering a wide academic window • Inclusion in the world • Make plans do-able • Understand your belief-systems • Dynamic behavior (“parenting”) plan • Medical management
Use of positive consequences to insist the child’s participation • Autonomy (doing as they please) • Attention (eye contact, body posture, proximity, being silly, etc.) • Verbalizing toward child (i.e., yelling at them, praise, singing a song to them, etc.) is highly reinforcing! • Any desired objects (i.e., favorite toys) • Any desired activity (trips, games, places, etc.) • Token systems and “markers” of impending rewards
Use of negative consequences (“penalties”) to insist on the child’s participation • Ignoring minor or low priority actions • Verbal redirection • Physical redirection (blocking & proximity management) • Removal of rewards/autonomy (all forms of “time-out” or “response cost”) • Physical escorts, hand-over-hand requirement (“over-correction”) • Restitution (righting the environment) • Restrictive-location time-out (bedroom/high chair) • Physical restraint (using appropriate training protocols such as “Prevention & Management of Aggressive Behavior” (PMAB))
The “positive behavioral supports” are those… • … done proactively (and sometimes reactively); • … non-contingently; • … regulated with the willingness or choosing of the child.
“Positive behavioral supports” are not… • … anything that involves a contingency! • Cardinal rule of Operant Condition: create a state of “want or desire” by depriving the person of the putative reinforcer. • Only give access to reinforcer when it has been “earned.” • This type of contingent “relationship” (between child and gate keeper of the rules) is – by definition – a form of “power assertion” (and not very fun if you are on the low end of the relationship).
TIMING!!!!!!!!!!!!!!!!Timing of response to appropriate behavior • Frequency and predictability in giving rewards • Only ask the child to give you a behavior that is in their repertoire • "Fading" and "thinning" of rewards
TIMING!!!!!!!!!!!!!!!!Timing of response to inappropriate behavior • Immediacy and certainty: be “startling” • Startle is very compelling • Use this to convey “important messages” • Use this to “insist” that you be attended to • The importance of brevity and frequency • Adult responses are moments in duration (duration of a startle) • Adult responds as often as possible to behavior
TALKING!!!!!!!!!!!!!!!!Verbal exchange around inappropriate behavior? • Say Nothing!!! Act first, then talk! • Talk AFTER the fact of a “penalty”, or during calm periods. • Vocal tones and facial expressions carry "the message": actively modulate your affect
Level 1.4: Communication • Discussions of feelings, thoughts, desires • Social-affective-emotional vocabulary • Social curricula with instruction in pragmatics • “Social grammar:” turn-taking, reading cues, etc. • Learn how to anticipate what others’ are saying • Learn how to interpret others’ feelings about what they are saying • Use commercially available curricula as instructional/therapeutic guide • Age-typical partners: don’t let your child’s only communication partners be adults and other children with developmental concerns • Rehearsal of social communication • Social stories • Social scripts • Video models and video self-monitoring
PROXIMITY!!!!!!!!!!!!!!!!Where are you standing in relation to behavior? • Be close enough to physically intervene if it is needed • talking (complaining, directing, repeating) from a distance is often reinforcing inappropriate behavior • paying attention to the child, yet too far away to physically intervene • The "riskier" the situation, the closer you should be standing • Practice giving your child some space • Set up routines in which you can come and go
Insisting of our children?INTERNAL CONSISTENCY • Are you "credible"? • Are you following your sense of right? • Say what you mean, mean what you say, do what you say you are going to do!