Download
1 / 20
200 likes | 387 Views
Skull Base Institute. Fully Endoscopic Vascular Decompression of the Trigeminal Nerve. Hrayr K. Shahinian M.D. Objectives. Brief review of surgical history Describe our endoscopic surgical procedure

E N D
Skull Base Institute Fully Endoscopic Vascular Decompression of the Trigeminal Nerve Hrayr K. Shahinian M.D.
Objectives • Brief review of surgical history • Describe our endoscopic surgical procedure • Demonstrate that endoscopy represents the next step forward in safe and effective vascular decompression of the trigeminal nerve
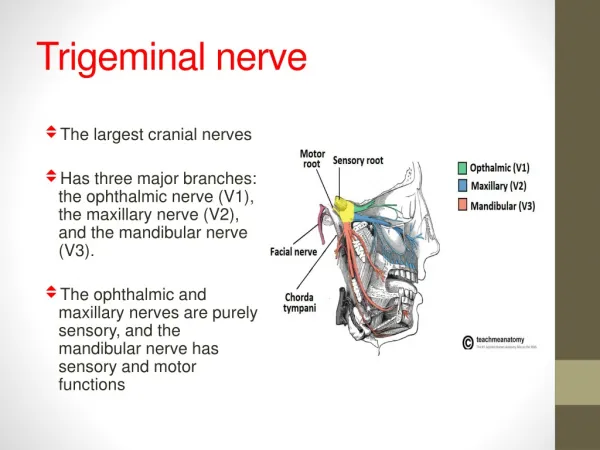
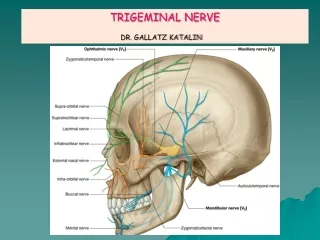
Trigeminal Neuralgia • A disease characterized by severe and often debilitating facial pain that occurs along the distribution of any of the three branches of the trigeminal nerve. • Incidence 4/100,000
Etiology • Historic Theories: • Early Surgical Pioneers: - Dandy- 1934 - Gardner- 1960’s - Jannetta- 1967 - Present
Historic Theories • Historical theories as to the etiology of TGN include bony deformities of the skull, abnormalities of the trigeminal nerve nuclei, carotid trauma to the gasserian ganglion, and mandibular misalignment.
Early Surgical Pioneers • Dandy in 1934 first hypothesized that vascular compression could be the cause of trigeminal neuralgia. • Gardner in the early 1960s helped to confirm this theory and was among the first surgeons to perform vascular decompression surgery for TGN.
Early Surgical Pioneers • Janetta in late 1960s and early 1970s proposed that TGN was caused by anatomic conflicts between blood vessels compressing the root entry zone (REZ) of the trigeminal nerve, providing us with our current understanding as to the pathogenesis of this disease. • It was at this time that the operating microscope was also introduced to vascular decompression surgery. (MVD)
Early Surgical Pioneers • Over the past 30 years several large series reports demonstrating a 70-80% long-term success rate for MVD have established that the overwhelming majority of cases of TGN are due to abnormal compression of the REZ of the trigeminal nerve by vessels of the posterior circulation. • With this high rate of success, minimal morbidity and almost no mortality, MVD has become the gold standard surgical treatment for TGN.
So Why Change the Current Standard Surgical Treatment for Trigeminal Neuralgia?
Limitations of MVD • Initial Failures • Recurrences • Complications • Primarily attributed to: - Incomplete ID - Incomplete decompression
History of CPA Endoscopy • Doyen- 1917 endoscopic rhizotomy • Mid 1990’s – Jennings, Magnan,O’Donoghue, and O’Flynn documented CPA anatomy • 1994 – Magnan publishes endoscope-assist MVD for TGN • 1997 – SBI began using a combined micro-endo. approach • 1998 – SBI converted to a fully endoscopic procedure
Endoscopic Advantages • Spencer- 1999 volume of view endoscope vs. microscope • Magnan- 1997 endoscopic assist for HFS 72% accuracy • Jarrahy- 1999 endoscopic assist for TGN - 24% of conflicts missed with microscope alone • Recognition of additional, often-obscured, nerve compression should improve outcomes
Endoscopic Vascular Decompression Start Video
Endoscopic Vascular Decompression Operation • Park bench position • 3 cm retroauricular incision • 1.5-2.0 cm retrosigmoid craniotomy • 4 mm 00 Hopkins rod rigid endoscope with irrigating sheath introduced through the crainiotomy
Endoscopic Vascular Decompression Operation • Without retraction the endoscope “turns the corner” to visualize structures of the cerebellopontine angle • Panoramic view of trigeminal nerve from pons to Meckel’s cave • Allows inspection from various angles to completely identify vascular conflicts
Endoscopic Vascular Decompression Operation • Holding arm locks endoscope into position allowing manipulation of instruments with both hands • Following the separation of the nerve and vessels, a 300 endoscope is advanced to re-survey the trigeminal nerve • Visualization of any additional conflicts are likewise dissected
Endoscopic Vascular Decompression Operation • Holding arm locks endoscope into position allowing manipulation of instruments with both hands • Following the separation of the nerve and vessels, a 300 endoscope is advanced to re-survey the trigeminal nerve • Visualization of any additional conflicts are likewise dissected
Endoscopic Vascular Decompression Operation • Teflon pledgets introduced between the vessel and nerve • Fibrin glue to secure pledgets • Craniotomy is closed • Dura re-approximated • Skin and subcutaneous tissues closed in layers
Post-op • Patients wake up in the operating room and are taken to the ICU for overnight monitoring • Most patients are home by post-operative day #2
Post-op • Patients are weaned from their pain medication regimen and are generally off all medication • Follow up in office