Download
1 / 36
580 likes | 2.04k Views
Lacrimal System Disorders. Dr. Landgraf Fall 2008. Overview. Readings Required Kanski, Chapter 5, 151-160, 162-164 “You Luck Out” B&J, Chapter 24, 415-435 “Springboard”. Overview. Dacryoadenitis Dry Eye Syndrome Punctal plugs Epiphora Dilation and Irrigation Punctal Disorders

E N D
Lacrimal System Disorders Dr. Landgraf Fall 2008
Overview • Readings • Required • Kanski, Chapter 5, 151-160, 162-164 • “You Luck Out” • B&J, Chapter 24, 415-435 • “Springboard”
Overview • Dacryoadenitis • Dry Eye Syndrome • Punctal plugs • Epiphora • Dilation and Irrigation • Punctal Disorders • Canalicular Disorders • Dacryocystitis
So do we need to review Dry Eye? • Quiz: To Avoid Staff Doctor Grief • What is needed for the diagnosis? • Hx? + • TBUT • NaFl • Lissamine green vs. Rose Bengal
So do we need to review Dry Eye? • Quiz: To Avoid Staff Doctor Grief • Tear volume tests • < 10 mm in 5 minutes? • Aqueous deficiency • With anesthetic? • < 5 mm in 5 minutes • Color change from yellow to red? • After 15 seconds < 10 mm • > 20 mm after 15 secondLet’s Ask _____?
Let’s Ask _____ • So do we need to review Dry Eye?
Save Some Tears • Punctal Occlusion • Temporary or permanent • Collagen aid with diagnosis • Silicone aid with more “permanent” occlusion
Save Some Tears • A few comments • Who typically has dry eye? • Something to think about • Punctum size with age • Legal troubles for the moneymaker • Extracanalicular vs intracanalicular
Save Some Tears • Overall Regimen • Make the diagnosis • Review the options • Artificial tears • “soft steroids” • Restasis • Temporary Permanent occlusion • Laser, cautery, lateral tarsorrhaphy
Save Some Tears • If you and your patient opt for plugs • Collagen first • Improvement in sxs, followed by worsening of sxs • No epiphora • Consider permanent
Save Some Tears • The Procedure per NBEO and your LAB Practical • Additionally, I dilate the punctum first prior to insertion • Practice taking them out of pack, and manipulating them • Know your lacrimal system anatomy
Save Some Tears • Complications • Canaliculitis • Epiphora • Dilation and irrigation (D & I) if intracanalicular • Loss • Discomfort or cosmetically displeasing • If extracanalicular
Save Some Tears • Plug Varieties • Dissolvable • Usually less than a week • Up to 6 months • Multiple sizes
Save Some Tears • Plug Varieties • Smart Plug • Long term reversible • “one size fits all” • Intracanalicular • Form Fit • Long term reversible • “one size fits all”
Save Some Tears • Plug Varieties • Nondissolvable (silicone) • Permanent reversible • 0.4-0.8 mm, may be “pre-loaded” or use forceps • Cap that protrudes from punctum
Save Some Tears • Making your office choice…considerations • Can I get it out easy if needed? • Always be methodical in your approach • Step-up option: diagnosistears and other optionscollagenpermanent
Dacryoadenitis • What is it? • Inflammation of the Lacrimal Gland • Superior lateral eyelid and adjacent adnexal swelling • S-shaped ptosis • Injection of lacrimal gland and surrounding conjunctiva • Rare
Dacryoadenitis • Etiologies • If acute, think… • Viral and bacterial • If chronic, think… • Sarcoid, TB, Graves’ etc. • Lacrimal gland tumor
Dacryoadenitis • Management • Acute: oral steroids • Culture and sensitivities if suspect bacterial • Keflex 500 mg qid po • Amoxicillin 250-500 mg tid po • Supportive if viral • Rest, ice, oral anlagesics • Sounds like recognition and a consult
Epiphora • You will see this one! • What is it? • Spilling of the tears over the lid margin • Rule-outs: • Dry Eye • Congenital naso-lacrimal duct obstruction • Apositional punctal problem • Block in lacrimal drainage system
Epiphora • Congenital NLD obstruction • Valve of Hasner not completely open at birth • 6% of infants • May look like conjunctivitis / dacryocystitis • Spontaneous resolution usually within months
Epiphora • Congenital NLD obstruction • Management • Hydrostatic massage • Finger occlusion and finger massage over sac and downward • Probing at 3-4 months if needed • Surgery at 21 months if needed • Always check for megalocornea
Epiphora • Adults: differential diagnosis • Dry eye? • Visible puncta without lid manipulation? • Ectropian • Visible obstruction? • Punctal regurgitation with pressure? • Other punctal diosrders • Atresia: congenital punctal stenosis • Vs acquired punctal stenosis: aging, allergy, infection, trauma
Epiphora • None of the above • Evaluation of remainder of lacrimal system • Usually monocular
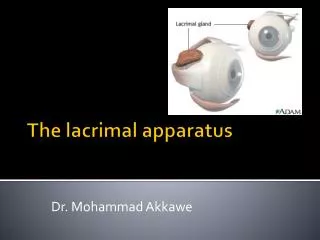
Epiphora • Evaluation of lacrimal drainage • Jones Testing • Equipment • Lacrimal dilator • “Lacrimal irrigation apparatus” • 2-5ml syringe + 23 gauge cannula • D & I = Dilation and Irrigation
Epiphora • Evaluation of lacrimal drainage • Jones I • NaFl in “virgin eye” • After 5 minutes, observe amount of NaFl remaining • If lacrimal drainage system normal, expect little remaining dye in and around eye • “Positive Jones I”
Epiphora • Evaluation of lacrimal drainage • Jones I: confirmation • Look for NaFl in back of throat • Look for Nafl “clearing of nose of white tissue” • Does any OD really do this? • Patent lacrimal system if dye present • “Positive Jones I”
Epiphora • Evaluation of lacrimal drainage • Jones II indications • Significant amount of dye present in eye after 5 minutes • No dye on tissue or in back of throat • “Negative Jones I” • Obstruction of lacrimal drainage system assumed beyond punctum
Epiphora • Evaluation of lacrimal drainage • Jones II Procedure • Anesthetize punctum • Dilate punctum • Down 2 and in 1-2 mm • Insert saline filled lacrimal apparatus syringe • Down 2 and in 1-2 mm • Inject 1-2 mm of saline
Epiphora • Evaluation of lacrimal drainage • Jones II Results • No fluid exits: complete blockage • Surgical consult for DCR (dacryocystorhinostomy) / punctoplasty • “Negative Jones II”
Epiphora • Evaluation of lacrimal drainage • Jones II Results • Fluid exits through upper punctum • Common canalicular block • “Negative Jones II”
Epiphora • Evaluation of lacrimal drainage • Jones II Results • Fluid exits through the nose • Patient tastes saline in back of throat (alternatively, effluent can be caught in basin) • Distal obstruction pushed through • Success! • “Postive Jones II”
Dacryocystitis • What is it? • Painful swelling over the lacrimal sac • Hyperemia • Epiphora
Dacryocystitis • What causes it? • Usually staph or pseudomonal related • Rarely a tumor • Epithelial carcinoma / lymphoma • Less pain • Silicone plug association
Dacryocystitis • Management • Hot compresses and daily massage • Oral antibiotic • Choices and why? • 10-14 days • D & I later after resolution • Consult and culture if recalcitrant